Professional Documents
Culture Documents
Topics in Obstetrics & Gynecology Volume 36 Issue 2 2016 (Doi 10.1097/01.pgo.0000479468.64386.d6) MacGregor, Caitlin Cronin, Beth - Evaluation and Management of Adnexal Masses
Topics in Obstetrics & Gynecology Volume 36 Issue 2 2016 (Doi 10.1097/01.pgo.0000479468.64386.d6) MacGregor, Caitlin Cronin, Beth - Evaluation and Management of Adnexal Masses
Uploaded by
Ricky Eko Januar SilaenOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Topics in Obstetrics & Gynecology Volume 36 Issue 2 2016 (Doi 10.1097/01.pgo.0000479468.64386.d6) MacGregor, Caitlin Cronin, Beth - Evaluation and Management of Adnexal Masses
Topics in Obstetrics & Gynecology Volume 36 Issue 2 2016 (Doi 10.1097/01.pgo.0000479468.64386.d6) MacGregor, Caitlin Cronin, Beth - Evaluation and Management of Adnexal Masses
Uploaded by
Ricky Eko Januar SilaenCopyright:
Available Formats
VOLUME 36 • NUMBER 2 www.topicsinobgyn.
com January 31, 2016
TOPICS IN
OBSTETRICS & GYNECOLOGY
Practical CME Newsletter for Clinicians
Evaluation and Management of Adnexal Masses
Caitlin MacGregor, MD, and Beth Cronin, MD
Learning Objectives: After participating in this CME activity, the obstetrician/gynecologist should be better able to:
1. Demonstrate understanding of the differential diagnosis and initial workup of adnexal masses.
2. Implement appropriate imaging follow-up and understand the role and limitations of biomarker screening.
3. Identify patients who warrant referral to a gynecologic oncologist.
Key Words: Adnexal mass, Biomarkers, Ultrasonography
Adnexal masses, defined as masses of the ovary, fallo- workup and evaluation of new adnexal masses and lead to
pian tube, or surrounding connective tissue, are a common more effective referral to a gynecologic oncologist. Finding
problem encountered in routine gynecologic practice. In the the proper balance of appropriate referral without overtest-
United States, up to 300,000 women are hospitalized, and ing and performing unnecessary surgery is a key component
60,000 surgeries are performed annually, for evaluation of of workup and evaluation of patients with adnexal masses.
an adnexal mass.1 Most women are diagnosed with benign
conditions; however, epithelial ovarian cancer (EOC) is First Steps of Evaluation: Developing a
identified in up to 20% of these patients.2 The risk of devel- Useful Differential Diagnosis
oping ovarian cancer in a woman’s lifetime is approximately Workup and evaluation of an adnexal mass may be prompted
1 in 70. Although the 5-year survival rate in women diag- by patient symptoms, incidental findings on workup for
nosed with stage I ovarian cancer exceeds 90%, only 20% another issue, or physical examination findings on routine
of cancers are detected at this early stage. The majority of examination. Thinking through the first steps of an evaluation
EOC is diagnosed at advanced stage, when the 5-year sur- requires attention to differential diagnosis, which can be a
vival rate ranges from 30% to 55%.3 broad list of conditions.
There is clear evidence that women with EOC have Adnexal masses, although much less common in children
decreased morbidity and improved survival when surgeons and adolescents than in reproductive-age women, may be
experienced in gynecologic oncology cases perform the consistent with malignancy. The most common type of ovar-
initial surgery.4 However, there is a gap in the ideal manage- ian malignancy in this population is germ cell tumors. In
ment of such patients when referral or consultation with a neonates, a physiologic cyst from maternal hormone stimu-
gynecologic oncologist is not sought preoperatively. This lation will typically resolve by 6 months of age. After the
goal of this article is to address this gap by reviewing the neonatal period and before adolescence, physiologic cysts
patient risk factors, physical examination findings, imaging are generally not seen, but when present are often the result
modalities, and serum markers that should guide the initial of enlargement of a cystic follicle. In adolescents, the devel-
opment of simple and complex cysts is much more common,
Dr. MacGregor is Clinical Instructor of Obstetrics and Gynecology, and Dr. Cronin
is Assistant Professor (Clinical) of Obstetrics and Gynecology, Warren Alpert with the differential diagnosis expanding to include imperfo-
Medical School of Brown University, Women & Infants Hospital, 101 Dudley St, rate hymen or noncommunicating uterine horn, cystadenomas,
Providence, RI 02906; E-mail: bcronin@wihri.org. paratubal cysts, hydro or pyosalpinx, ectopic pregnancies, and
The authors and all staff in a position to control the content of this CME activity appendicitis. As in adults, ultrasonography is the primary
and their spouses/life partners (if any) have disclosed that they have no financial
relationships with, or financial interests in, any commercial organizations per- tool for initial evaluation. The use of biomarkers, and
taining to this educational activity. improvements in radiographic imaging as part of the initial
Lippincott Continuing Medical Education Institute, Inc., is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical
education for physicians.
Lippincott Continuing Medical Education Institute, Inc., designates this enduring material for a maximum of 2.0 AMA PRA Category 1 Credits™. Physicians should
only claim credit commensurate with the extent of their participation in the activity.
To earn CME credit, you must read the CME article and complete the quiz and evaluation on the enclosed answer form, answering at least seven of the 10 quiz questions
correctly. This activity expires on January 30, 2017.
1
PGOv36n2.indd 1 12/18/15 4:06 PM
Topics in Obstetrics & Gynecology January 31, 2016
evaluation of complex adnexal masses, has be required to facilitate the evaluation should
EDITORS facilitated a more conservative approach to be provided.
William Schlaff, MD the management of neoplasms in children Ectopic pregnancy generally presents as a
Professor and Chair, and adolescents. Ovarian preservation is the missed menstrual period in the setting of pel-
Department of Obstetrics standard of care except in the setting of a vic pain and/or vaginal bleeding. The finding
and Gynecology, Thomas
Jefferson Medical College,
cancer diagnosis. of an adnexal mass in a pregnant patient
Philadelphia, Pennsylvania In premenopausal women, gynecologic without a confirmed intrauterine pregnancy
causes of an adnexal mass include acute should be considered an ectopic pregnancy
Lorraine Dugoff, MD pathologic processes such as ovarian torsion, until proven otherwise. Immediate evaluation
Associate Professor and Chief, tubo-ovarian abscess (TOA), and ectopic preg- and treatment are required for this poten-
Division of Reproductive
Genetics, Department of
nancy. Chronic or nonacute causes include a tially life-threatening condition. Sonographic
Obstetrics and Gynecology, functional or corpus luteal cyst (most com- evidence suggestive of an ectopic preg-
University of Pennsylvania monly); endometrioma; uterine leiomyoma; nancy includes lack of yolk sac or fetal pole
Perelman School of or a benign ovarian neoplasm such as a der- within the uterine cavity, a noncystic adnexal
Medicine, Philadelphia,
moid cyst. Gastrointestinal manifestations mass, and possibly echogenic peritoneal
Pennsylvania
such as diverticulitis, appendicitis, peritoneal free fluid.
or omental cysts, or malignancy also should Ovarian torsion is caused by complete or
FOUNDING EDITORS be considered. Metastases from other pri- partial rotation of the ovary on its support
Edward E. Wallach, MD mary cancers must be included in the dif- ligaments, which often impedes its vascular
Roger D. Kempers, MD ferential diagnosis.1 Differential diagnosis in supply. Common causes of torsion include
postmenopausal women is similar, aside from ovarian cysts, neoplasms, elongated utero-
exclusion of pregnancy-related causes. ovarian ligament, and pregnancy. Rotation of
ASSOCIATE EDITORS
the ovary’s vascular pedicle, the infundibu-
Meredith Alston, MD
Acute Presentation of Adnexal lopelvic ligament, causes compression of
Denver, Colorado Masses both lymphatic and venous outflow and arte-
Samantha Buery-Joyner, MD
Case 1. A 22-year-old G0 presents with rial inflow. Arterial flow is impeded less,
Falls Church, Virginia
acute onset of right lower quadrant pain. which ultimately leads to ovarian swelling
She notes severe pain that started 2 hours and enlargement followed by ischemia and
Nancy D. Gaba, MD ago. She notes nausea. She does not have necrosis if left untreated. An ovarian mass is
Washington, DC vomiting or fever. the primary risk factor for torsion, with ovar-
Jennifer Goedken, MD
For women presenting emergently with ian size greater than 5 cm increasing risk.5
Atlanta, Georgia
lower abdominal pain, adnexal mass Presenting symptoms of ovarian torsion
should be high on the list of differential include pelvic pain, adnexal mass, nausea
Veronica Gomez-Lobo, MD diagnoses. In the acute setting, this list and vomiting, fever, and vaginal bleeding.
Washington, DC should include ovarian torsion, ectopic On ultrasonography, the torsed ovary may be
pregnancy, ruptured cyst, TOA, and nongy- rounded and enlarged compared with the
Star Hampton, MD
necologic issues such as appendicitis. The contralateral ovary and may display hetero-
Providence, Rhode Island
initial workup in these cases should involve geneous stroma secondary to edema and
Enrique Hernandez, MD a full history and physical examination, hemorrhage. Decreased or absent Doppler
Philadelphia, Pennsylvania pregnancy test, complete blood count, and flow within the ovary on 2-dimensional, color,
pelvic ultrasonography. Pain control as may and 3-dimensional Doppler ultrasonography
Nancy Hueppchen, MD
Baltimore, Maryland
Bradley S. Hurst, MD The continuing education activity in Topics in Obstetrics & Gynecology is intended for obstetricians, gynecologists, and other health
Charlotte, North Carolina care professionals with an interest in the diagnosis and treatment of obstetric and gynecological conditions.
Topics in Obstetrics & Gynecology (ISSN 2380-0216) is published 18 times per year by Lippincott Williams & Wilkins, Inc., 16522
Peter G. McGovern, MD Hunters Green Parkway, Hagerstown, MD 21740-2116. Customer Service: Phone (800) 638-3030, Fax (301) 223-2400, or
E-mail customerservice@lww.com. Visit our website at LWW.com. Publisher, Randi Davis.
New York, New York
Copyright © 2015 Wolters Kluwer Health, Inc. All rights reserved. Priority Postage paid at
Owen Montgomery, MD Hagerstown, MD, and at additional mailing offices. POSTMASTER: Send address changes
to Topics in Obstetrics & Gynecology, Subscription Dept., Lippincott Williams & Wilkins,
Philadelphia, Pennsylvania P.O. Box 1600, 16522 Hunters Green Parkway, Hagerstown, MD 21740-2116.
PAID SUBSCRIBERS: Current issue and archives from 2004 on are now available FREE online at www.topicsinobgyn.com.
Christopher M. Morosky, MD
Subscription rates: Personal: US $501, international $700. Institutional: US $1157, international $1356. In-training: US resident $146
Farmington, Connecticut with no CME, international $169. GST Registration Number: 895524239. Send bulk pricing requests to Publisher. Single copies: $74.
COPYING: Contents of Topics in Obstetrics & Gynecology are protected by copyright. Reproduction, photocopying, and storage or
William D. Petok, PhD transmission by magnetic or electronic means are strictly prohibited. Violation of copyright will result in legal action, including civil and/or
Baltimore, Maryland criminal penalties. Permission to reproduce copies must be secured in writing; at the newsletter website (www.topicsinobgyn.com),
select the article, and click “Request Permission” under “Article Tools” or e-mail customercare@copyright.com. Reprints: For com-
James M. Shwayder, MD, JD mercial reprints and all quantities of 500 or more, e-mail reprintsolutions@wolterskluwer.com. For quantities of 500 or under,
e-mail reprints@lww.com, call 1-866-903-6951, or fax 1-410-528-4434.
Jackson, Mississippi Opinions expressed do not necessarily reflect the views of the Publisher, Editor, or Editorial Board. A mention of products or services does
not constitute endorsement. All comments are for general guidance only; professional counsel should be sought for specific situations.
PGOv36n2.indd 2 12/18/15 4:06 PM
January 31, 2016 Topics in Obstetrics & Gynecology
suggests torsion. The sensitivity of ultrasonography ranges were to improve patient care, decrease unnecessary imag-
from 46% to 75% for the diagnosis of ovarian torsion and is ing, and reduce patient anxiety.8 In premenopausal women,
made more sensitive when combining multiple sonographic simple cysts smaller than 10 cm are almost always benign.
findings, such as abnormal ovarian location, free fluid, and Simple cysts larger than 3 cm should be described in the
abnormal blood flow.6 Diagnosis of ovarian torsion is clinical, imaging report. Simple cysts 5 cm or smaller are normal
made from a combination of history, physical, and possibly and do not require ultrasonographic follow-up, whereas
sonographic findings. However, a clear story and concerning those larger than 5 cm should be followed yearly with ultra-
examination results in the absence of ultrasonographic find- sonography. If a simple cyst is larger than 7 cm, it may be
ings to suggest torsion should not halt surgical evaluation if difficult to assess completely with ultrasonography; further
suspicion is high, as that is the only way to make a definitive imaging with MRI, or surgical excision, is indicated. In
diagnosis. postmenopausal women, simple cysts 1 cm or smaller in
Classic presentation of a ruptured cyst is acute onset of size are clinically inconsequential and do not require fol-
pelvic pain in the mid-menstrual cycle, typically after inter- low-up. However, yearly follow-up is warranted if a simple
course. Free fluid in the adnexa or posterior cul-de-sac is cyst is between 1 cm and 7 cm in size, with the option to
generally seen on ultrasonography. A cyst may become hem- decrease frequency of ultrasonography once stability is
orrhagic without rupture. If there is concern for brisk bleeding documented. Simple cysts larger than 7 cm should be man-
causing anemia or hemodynamic instability, surgical inter- aged similarly to those in premenopausal women.
vention is indicated, but in general, a ruptured cyst can be Complex cysts are generally benign and are most often
managed conservatively if adequate pain control is attained. characterized as hemorrhagic cysts, endometriomas, or der-
TOA is also a cause of acute onset of abdominal pain. Its moid cysts. The classic ultrasonographic feature of hemor-
course is generally more indolent, and often patients present rhagic cysts is a reticular pattern of echoes that has a lacy
with fever, chills, vaginal discharge, lower abdominal pain, appearance secondary to fibrin deposition. These should
and an adnexal mass. Ultrasonographic findings consistent resolve without intervention; however, if larger than 5 cm,
with TOA include a complex, multilocular mass that can they should be re-imaged within a short interval (6–12
obliterate the normal adnexal anatomy, with fluid-contain- weeks) to ensure resolution. Given that hemorrhagic cysts are
ing internal echoes representing internal debris.7 Timely the result of ovulation, frankly menopausal patients should
initiation of treatment with broad-spectrum antibiotics and not have hemorrhagic cysts; if found, surgical evaluation
possible drainage is necessary to prevent sepsis or further should be considered. Perimenopausal and newly menopau-
damage to the adnexa. In the case of an unstable patient sal patients will occasionally ovulate, and short-interval fol-
with findings concerning for ruptured TOA, surgical evalu- low-up is recommended to ensure resolution (regardless of
ation is the first-line treatment. size) rather than surgical evaluation.
Case 1 disposition. First steps in management include Endometriomas generally demonstrate internal, homoge-
physical examination, pregnancy test, ultrasonography, and neous, ground-glass echoes without internal Doppler flow,
pain control as indicated. wall nodules, or other neoplastic features. Initially, short-
interval follow-up with ultrasonography is recommended
Nonacute Presentation of Adnexal Masses to exclude hemorrhagic cysts, followed by yearly ultra-
Case 2. A 32-year-old G1P1001 presents for her annual sonographic follow-up. Approximately 2.5% of endome-
examination. She is noted to have some fullness on pelvic triomas are malignant, although this is mostly in women
examination. This is a nonacute presentation of an adnexal
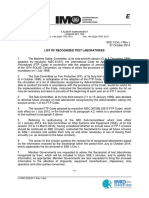
mass. Table 1. Summary of Recommendations for Simple Cysts
Premenopausal Postmenopausal
Imaging
≤3 cm: normal finding, does not <1 cm: clinically inconsequential,
Transvaginal ultrasonography is currently the most com- need follow-up, no need to does not need follow-up
mon and preferred initial imaging modality to evaluate describe in report
adnexal masses. Premenopausal ovaries vary in appearance >3 cm and ≤5 cm: describe in >1 cm and ≤7 cm: describe in report
throughout the menstrual cycle. Follicles appear as multi- report as almost certainly as almost certainly benign, yearly
ple, thin, smooth-walled, round or oval, anechoic spaces benign, does not need follow-up initially, may continue
with no flow on Doppler studies. Multiple developing fol- follow-up yearly or decrease when stable
or decreased in size
licles then become one or more dominant follicle. The
dominant follicle, generally 2 to 2.4 cm at ovulation, >5 cm and ≤7 cm: describe in
report as almost certainly
becomes a corpus luteum after ovulation. In contrast, follicu-
benign, yearly follow-up with
logenesis has ceased in the postmenopausal ovary. Overall ultrasonography
volume is decreased, and the postmenopausal ovary appears
>7 cm: difficult to assess >7 cm: MRI or surgical evaluation
homogeneous in echotexture. completely with
In October 2009, the Society of Radiologists in Ultrasound ultrasonography, further
met to develop an evidence-based consensus statement imaging with MRI or surgical
regarding definitive recommendations for monitoring evaluation
adnexal ultrasonographic findings (Table 1). The goals Adapted from Levine et al.8
PGOv36n2.indd 3 12/18/15 4:06 PM
Topics in Obstetrics & Gynecology January 31, 2016
older than 45 years with endometriomas larger than 9 cm.9 less invasive, and provides diagnostic results sooner than
Development of solid components or a rapid increase in surgical intervention. However, aspiration is contraindicated
size should be a red flag for clinicians. in postmenopausal women, especially when there is concern
Classic ultrasonographic features of dermoid cysts (mature for malignancy. The sensitivity of diagnostic cytology to
cystic teratomas) are focal or diffuse hyperechoic compo- detect malignancy ranges from 25% to 82%.12
nents, hyperechoic lines, an area of acoustic shadowing, and Case 2 disposition. You perform ultrasonography, which
absent internal Doppler flow. These findings reflect a der- shows a 4-cm simple cyst. Follow-up imaging is not
moid’s cystic and mature tissue composition such as skin, required in this premenopausal woman with a simple cyst
hair follicles, sebaceous glands, and muscle. Dermoid cysts smaller than 5 cm.
are bilateral in 10% to 17% of cases. Ultrasonographic fol-
low-up is recommended every 6 to 12 months to ensure size Biomarkers
stability. Indeterminate features should be followed more Serum biomarkers can be a useful addition to the initial
closely. Postmenopausal women with features of dermoids workup and evaluation of new adnexal masses in helping to
should be referred for surgical evaluation. The rate of distinguish benign from malignant disease. CA-125 is a
malignant components in a dermoid cyst is about 0.2% to glycoprotein produced by the mesothelial cells lining the
2%, with women older than 50 years and with tumors larger peritoneum, pericardium, and pleura, which is elevated in
than 10 cm most likely to be affected.10 Features that are approximately 80% of women with EOC.13 However, only
concerning for malignancy include isoechoic branching 50% of patients with stage I disease have an elevated CA-125
structures, solid areas with flow, and evidence of invasion level at the time of diagnosis, thus precluding its use as a
into adjacent structures. In general, thick septations, solid screening test.14 Many conditions can cause an increase in
elements with internal flow, focal areas of wall thickening, CA-125 level, including menses, pregnancy, cirrhosis, ascites,
ascites, and nodularity are concerning for malignancy and congestive heart failure, acute or chronic pelvic inflamma-
warrant further investigation. tory disease, fibroids, and endometriosis. The reported sensi-
Peritoneal inclusion cysts and hydrosalpinges are also tivity of CA-125 testing to differentiate between benign and
common ultrasonographic findings seen in the evaluation for malignant adnexal masses ranges from 61% to 90%, with
adnexal masses. In general, peritoneal inclusion cysts are seen specificity ranging from 35% to 91%.1
in women with a history of abdominal or pelvic surgery, pel- With regard to nongynecologic etiology, both carbohy-
vic inflammatory disease, or endometriosis. On ultrasonogra- drate antigen 19-9 (CA 19-9) and carcinoembryonic antigen
phy, a peritoneal inclusion cyst appears as a cystic mass that (CEA) are helpful biomarkers. CA 19-9 level can be ele-
follows the contour of adjacent pelvic organs, with the ovary vated in association with gastric, gallbladder, and pancreatic
at its edge or suspended within the mass. If ultrasonographic cancers. CEA level can be raised in patients with mucinous
findings are classic for an inclusion cyst, no further follow-up cancers associated with the gastrointestinal tract or ovary.
is indicated. Hydrosalpinges appear as tubular-shaped cystic Elevated serum CEA can be documented in patients with
masses that may have short, round projections or indentations breast, pancreas, thyroid, and lung malignancies. Other condi-
on opposite sides of the mass. In general, they should be tions associated with elevated CEA level include pancreatitis,
separate from the ipsilateral ovary. Similar to peritoneal inclu- inflammatory bowel disease, pancreatitis, diverticulitis, chol-
sion cysts, if there are classic features for hydrosalpinx, no ecystitis, pulmonary infection, liver cirrhosis, cigarette smok-
follow-up is indicated unless symptoms develop. However, if ing, and mucinous cystadenoma of the appendix or ovary.15
the patient also presents with infertility, referral to a reproduc- Various tools are available that combine serum biomark-
tive endocrinologist is indicated. ers with ultrasonographic findings to calculate preopera-
CT and MRI are not recommended for the initial workup tive risk of malignancy; however, none have been widely
of adnexal masses. These modalities should be reserved for adopted at this point. The Risk of Ovarian Cancer Algorithm
specific indications, such as use of CT to evaluate the abdo- (ROCA) categorizes women as at low, intermediate, and
men for metastases when cancer is suspected on the basis of high risk, and recommendations for care are stratified into
ultrasonographic findings, physical examination, or serum annual follow-up, repeat serum CA-125 testing, or trans-
biomarkers. Peritoneal implants, pelvic and periaortic lym- vaginal ultrasonography, depending on score.16 The Prostate,
phadenopathy, omental caking, obstructive uropathy, and a Lung, Colorectal and Ovarian Cancer Screening Trial was
possible different primary cancer site are all examples of a large randomized controlled trial that evaluated the effect
important CT findings. MRI may have superior ability on mortality of screening with CA-125 testing and trans-
compared with transvaginal ultrasonography at classifying vaginal ultrasonography. There were an increased number
malignant masses, although the data are limited, and overall of ovarian cancer diagnoses in the intervention group com-
there is a lower detection rate.11 Expense and inconvenience pared with the usual care group, but the screening interven-
are frequent barriers to the use of these modalities. During tion had no effect on mortality rate. An increased rate of
pregnancy, MRI is a helpful modality to decrease radiation adverse effects was associated with diagnostic evaluation of
exposure to the developing fetus. women with false-positive screening results.17 At this time,
Ultrasound-guided aspiration of ovarian cysts for diagnosis the Society of Gynecologic Oncology (SGO) does not rec-
and treatment may seem to be a practical next step in the ommend routine CA-125 testing with or without trans-
workup of cystic adnexal masses. Indeed, it is less expensive, vaginal ultrasonography to screen low-risk women. SGO
PGOv36n2.indd 4 12/18/15 4:06 PM
January 31, 2016 Topics in Obstetrics & Gynecology
recommends that cost-effectiveness analysis be performed Although nonspecific, these symptoms are typically present
before a universal screening program is adopted.18 for less than a year and occur more than 12 days per month.
Ova1 is another tool developed to identify high-risk ovar-
ian tumors preoperatively. It measures CA-125, beta Pregnancy
2-microglobulin, transferrin, apolipoprotein A1, and tran- Before the widespread use of ultrasonography, many
sthyretin levels. OvaCalc software assigns a score on the adnexal masses went unrecognized during pregnancy
basis of menopausal status. In a trial of 516 women referred unless they became symptomatic. Now, many asympto-
for surgery for adnexal masses, sensitivity and specificity matic adnexal masses are seen on dating or growth ultra-
were 92.5% and 42.8%, respectively.19 A more recent study sonography in the first half of pregnancy. In addition to
of 590 women with various malignancies (including none- ectopic pregnancy, there are several adnexal masses that are
pithelial ovarian cancer, epithelial ovarian cancer, malig- uniquely associated with pregnancy.
nancies metastatic to the ovary, pelvic cancer, and border- Corpus luteal cysts are commonly seen with an early
line tumors), Ova1 had a higher sensitivity to detect ovarian intrauterine pregnancy and help support the growth of the
cancer than CA-125 level and physician assessment.20 developing pregnancy. Typically, these cysts are less than
Human epididymis protein 4 (HE4) is a newer serum 2.5 cm; however, they may become painful or enlarged
biomarker for EOC, which is overexpressed by EOC secondary to hemorrhage within corpus luteum. A luteoma
tumors, creating elevated serum levels. Its sensitivity is is a nonneoplastic ovarian change associated with the
similar to CA-125 level for detection of malignancy; how- increases of sex hormones, particularly of progesterone and
ever, it is much less likely to be elevated in benign condi- testosterone, during pregnancy that simulates a neoplasm
tions.21 An initial study by Moore et al22 led to the develop- on microscopic, gross, or clinical examination.26 Luteomas
ment of the Risk of Malignancy Algorithm (ROMA), which spontaneously involute postpartum and should be sus-
is a scoring system that incorporates serum levels of CA-125 pected in pregnant women with an adnexal mass and signs
and HE4 with menopausal status. ROMA score was evalu- of virilization. Theca lutein cysts are luteinized follicle
ated as a preoperative risk stratification tool and found to cysts associated with pregnancy. They result from over-
have sensitivity of 92.3% and specificity of 76% for detect- stimulation associated with high beta-HCG levels or
ing EOC in postmenopausal women, and it had 100% sen- increased sensitivity of beta-HCG. Suspicion for a theca
sitivity and 74.2% specificity in premenopausal women.22 lutein cyst should be raised in a pregnant woman with bilat-
In children and adolescents, there are additional biomark- eral multiseptated adnexal masses, multiple gestations,
ers for consideration. Alpha-fetoprotein is an oncofetal ovarian hyperstimulation, or gestational trophoblastic dis-
antigen found in endodermal sinus tumors, immature terato- ease. These cysts resolve spontaneously in the weeks to
mas, and mixed germ cell tumors. Lactate dehydrogenase months after removal of the beta-hCG source.
(LDH) level is often elevated in association with dysgermi- Other causes of adnexal masses are similar to those for
nomas. Human chorionic gonadotropin (hCG) level is ele- reproductive-age women. Asymptomatic adnexal masses in
vated in patients with embryonal ovarian carcinomas and pregnancy should be resected if they are larger than 10 cm in
nongestational choriocarcinoma. CEA can be elevated in diameter, solid, or contain solid or cystic areas with or with-
association with both epithelial or germ cell tumors. Inhibin- out septae, as these findings increase the likelihood of malig-
and müllerian-inhibiting substance levels are raised in nancy.27,28 Furthermore, resection of large adnexal masses,
patients with granulosa-theca cell tumors. regardless of whether the underlying cause is benign or
malignant, reduces the risk of torsion or rupture during preg-
Special Considerations nancy. The optimal timing of surgery for adnexal masses is
Patient History after the first trimester, when most functional cysts will
Specific patient risk factors should increase one’s suspi- resolve, organogenesis is complete, and placental takeover of
cion for malignancy. The incidence of malignancy increases hormonal production from the corpus luteum has occurred.
after menopause, with the median age of ovarian cancer
diagnosed at age 63 years.23 Family history of breast or Referral to Gynecologic Oncology
ovarian cancer is also important, with BRCA1, BRCA2, Research has shown that there is improved morbidity and
and hereditary nonpolyposis colon cancer syndrome (Lynch mortality when patients diagnosed with EOC have their ini-
syndrome) being the most prominent, increasing the tial surgery performed by a gynecologic oncologist. Guidelines
patient’s risk of ovarian malignancy 60-, 30-, and 13-fold, for referring a woman with a new pelvic mass to gynecologic
respectively.24 Other considerations are nulliparity, early oncology have been created by both the American College of
menarche, late menopause, white ethnicity, endometriosis, Obstetricians and Gynecologists and SGO (Table 2).
and primary infertility. In contrast, bilateral salpingectomy, Im et al29 validated these referral guidelines in a study of
hysterectomy, multiparity, and use of oral contraceptives 1035 women who underwent surgery for a pelvic mass at 6
reduce the risk of ovarian cancer. referral centers. Primary ovarian cancers were found in
Goff et al25 established a list of symptoms commonly asso- 30.7% of the cases, and an additional 4.8% of patients had
ciated with ovarian cancer, which includes pelvic or abdom- metastases to the ovary. The referral guidelines captured
inal pain, increased abdominal size or bloating, early satiety 70% of malignancies in premenopausal women and 94% in
or difficulty eating, and urinary urgency or frequency. postmenopausal women.
5
PGOv36n2.indd 5 12/18/15 4:06 PM
Topics in Obstetrics & Gynecology January 31, 2016
REFERENCES
Table 2. SGO and ACOG Referral Guidelines for Patients With a
Newly Diagnosed Pelvic Mass 1. ACOG Practice Bulletin. Management of adnexal masses. Obstet Gynecol.
2007;110(1):201-214.
Premenopausal (<50 yrs)
2. Curtin JP. Management of the adnexal mass. Gynecol Oncol. 1994;55(3 Pt 2):
CA-125 >200 U/mL S42-46.
3. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2006. CA Cancer J Clin.
Ascites 2006;56(2):106-130.
Evidence of abdominal or distant metastasis (by examination or 4. Earle CC, Schrag D, Neville BA, et al. Effect of surgeon specialty on pro-
imaging) cesses of care and outcomes for ovarian cancer patients. J National Cancer
Inst. 2006;98(3):172-180.
Family history of breast or ovarian cancer (in a first-degree relative) 5. Houry D, Abbott JT. Ovarian torsion: a fifteen-year review. Ann Emerge
Med. 2001;38(2):156-159.
Postmenopausal (>50 yrs)
6. Mashiach R, Melamed N, Gilad N, et al. Sonographic diagnosis of ovarian tor-
CA-125 >35 U/mL sion: accuracy and predictive factors. J Ultrasound Med. 2011;30(9):1205-1210.
7. Wiesenfeld HC, Sweet RL. Progress in the management of tuboovarian
Ascites abscesses. Clin Obstet Gynecol. 1993;36(2):433-444.
Nodular or fixed pelvic mass 8. Levine D, Brown DL, Andreotti RF, et al. Management of asymptomatic ovar-
ian and other adnexal cysts imaged at US: Society of Radiologists in Ultrasound
Evidence of abdominal or distant metastasis (by examination or Consensus Conference Statement. Radiology. 2010;256(3):943-954.
imaging study) 9. Van Gorp T, Amant F, Neven P, et al. Endometriosis and the development
of malignant tumours of the pelvis. A review of literature. Best Pract Res
Family history of breast or ovarian cancer (in a first-degree relative)
Clin Obstet Gynaecol. 2004;18(2):349-371.
ACOG, American College of Obstetricians and Gynecologists; SGO, Society of 10. Comerci JT, Jr, Licciardi F, Bergh PA, et al. Mature cystic teratoma: a
Gynecologic Oncology. clinicopathologic evaluation of 517 cases and review of the literature. Obstet
Adapted from Im et al.29 Gynecol. 1994;84(1):22-28.
11. Sohaib SA, Mills TD, Sahdev A, et al. The role of magnetic resonance imag-
ing and ultrasound in patients with adnexal masses. Clin Radiol. 2005;60(3):
Conclusion 340-348.
12. Moran O, Menczer J, Ben-Baruch G, et al. Cytologic examination of ovar-
Management of a patient with an adnexal mass is a common ian cyst fluid for the distinction between benign and malignant tumors.
scenario for generalist obstetrician/gynecologists. Whether Obstet Gynecol. 1993;82(3):444-446.
13. Bast RC, Jr, Feeney M, Lazarus H, et al. Reactivity of a monoclonal anti-
identified incidentally on imaging for an unrelated issue, body with human ovarian carcinoma. J Clin Invest. 1981;68(5):1331-1337.
asymptomatically palpated on annual pelvic examination, or 14. National Institutes of Health Consensus Development Conference Statement.
found in the workup of acute pain, balancing the risks of Ovarian cancer: screening, treatment, and follow-up. Gynecol Oncol. 1994;
55(3 Pt 2):S4-14.
intervention with ensuring that women at high risk for malig- 15. Menon U JI. Principles and Practice of Gynecologic Oncology. Philadelphia,
nancy are appropriately referred to a gynecologic oncologist PA: Lippincott Williams & Wilkins; 2000.
should form the core of management. Transvaginal ultra- 16. Skates SJ. Ovarian cancer screening: development of the risk of ovarian
cancer algorithm (ROCA) and ROCA screening trials. Int J Gynecol Cancer.
sonography should be the first-line imaging modality for 2012;22(Suppl 1):S24-26.
diagnosis of adnexal masses, with CT and MRI saved for 17. Buys SS, Partridge E, Black A, et al. Effect of screening on ovarian cancer
unique circumstances. mortality: the Prostate, Lung, Colorectal and Ovarian (PLCO) Cancer
Screening Randomized Controlled Trial. JAMA. 2011;305(22):2295-2303.
18. Use of CA125 in Screening for Ovarian Cancer. Public Policy. 2010; http://
www.sgo.org/newsroom/position-statements-2/use-of-ca125-in-screening-
Clinical Pearls for-ovarian-cancer/. Accessed October 21, 2015.
19. Muller CY. Doctor, should I get this new ovarian cancer test-OVA1? Obstet
• Simple cysts as large as 10 cm in premenopausal Gynecol. 2010;116(2 Pt 1):246-247.
women are almost always benign, and they require 20. Ueland FR, Desimone CP, Seamon LG, et al. Effectiveness of a multivariate
intervention only in the setting of pain or discomfort. index assay in the preoperative assessment of ovarian tumors. Obstet
Gynecol. 2011;117(6):1289-1297.
• Acute presentation of pelvic pain requires expanding 21. Drapkin R, von Horsten HH, Lin Y, et al. Human epididymis protein 4
(HE4) is a secreted glycoprotein that is overexpressed by serous and endo-
the differential diagnosis, providing pain management, metrioid ovarian carcinomas. Cancer Res. 2005;65(6):2162-2169.
and performing appropriate workup. 22. Moore RG, Miller MC, Disilvestro P, et al. Evaluation of the diagnostic
accuracy of the risk of ovarian malignancy algorithm in women with a pel-
• CA-125 level can be falsely elevated in many circum- vic mass. Obstet Gynecol. 2011;118(2 Pt 1):280-288.
stances other than EOC, including menses, pregnancy, 23. SEER Stat Facts: Ovarian cancer. http://seer.cancer.gov/statfacts/html/
ovary.html. Accessed October 30, 2015.
cirrhosis, ascites, congestive heart failure, acute or 24. Finch A, Beiner M, Lubinski J, et al. Salpingo-oophorectomy and the risk
chronic pelvic inflammatory disease, fibroids, and of ovarian, fallopian tube, and peritoneal cancers in women with a BRCA1
endometriosis. or BRCA2 mutation. JAMA J Am Med Assoc. 2006;296(2):185-192.
25. Goff BA, Mandel LS, Drescher CW, et al. Development of an ovarian can-
• Referral guidelines have been developed to identify cer symptom index: possibilities for earlier detection. Cancer.
2007;109(2):221-227.
patients at high risk for malignancy who should be 26. Clement PB. Tumor-like lesions of the ovary associated with pregnancy. Int
evaluated by a gynecologic oncologist. J Gynecol Pathol. 1993;12(2):108-115.
27. Leiserowitz GS. Managing ovarian masses during pregnancy. Obstet Gynecol
• Pelvic masses in pregnancy are generally benign. Surv. 2006;61(7):463-470.
However, if there is any question or the size is large 28. Schmeler KM, Mayo-Smith WW, Peipert JF, et al. Adnexal masses in preg-
nancy: surgery compared with observation. Obstet Gynecol. 2005;105(5 Pt 1):
enough to warrant surgical evaluation, the second tri- 1098-1103.
mester is the ideal time. 29. Im SS, Gordon AN, Buttin BM, et al. Validation of referral guidelines for
women with pelvic masses. Obstet Gynecol. 2005;105(1):35-41.
PGOv36n2.indd 6 12/18/15 4:06 PM
January 31, 2016 Topics in Obstetrics & Gynecology
CME Quiz: Volume 36, Number 2
To earn CME credit, you must read the CME article and complete the quiz and evaluation on the enclosed answer form, answering at least
seven of the 10 quiz questions correctly. Select the best answer and use a blue or black pen to completely fill in the corresponding box
on the enclosed answer form. Please indicate any name and address changes directly on the answer form. If your name and address do
not appear on the answer form, please print that information in the blank space at the top left of the page. Make a photocopy of the completed
answer form for your own files and mail the original answer form in the enclosed postage-paid business reply envelope. Your answer form
must be received by Lippincott CME Institute by January 30, 2017. Only two entries will be considered for credit. At the end of each quarter,
all CME participants will receive individual issue certificates for their CME participation in that quarter. Participants will receive CME certificates
quarterly in April, July, October, and the fourth quarter in January of the following year. For more information, call (800) 638-3030.
Online quiz instructions: To take the quiz online, log on to your account at www.topicsinobgyn.com, and click on the “CME” tab at
the top of the page. Then click on “Access the CME activity for this newsletter,” which will take you to the log-in page for http://cme.lww.
com. Enter your username and password. Follow the instructions on the site. You may print your official certificate immediately. Please
note: Lippincott CME Institute, Inc., will not mail certificates to online participants. Online quizzes expire on the due date.
1. A 32-year-old G4P4 presents for annual examination. She 5. A 22-year-old woman presents to the emergency depart-
notes occasional pelvic pain and dyspareunia, with no signifi- ment with left-sided lower abdominal pain and spotting.
cant medical, surgical, or family history and no obvious masses She has regular cycles, and her last menstrual period was
or nodularity on examination. Ultrasonography demonstrates a 7 weeks previously. Her beta-hCG level is 2650. Two days
3.0-cm simple cyst on the right ovary, normal uterus, and left later, her beta-hCG level is 2790. No intrauterine preg-
adnexa. Which one of the following describes the appropriate nancy is seen on ultrasound, but a 2.5-cm, right adnexal,
next step? nonovarian mass is seen. The patient’s vital signs are all
A. Surgical evaluation normal. Which one of the following describes the appropri-
B. Repeat ultrasonography in 6 months ate next step?
C. Repeat ultrasonography in 1 year A. Check CA-125 level
D. Routine annual care. B. Treat for ectopic pregnancy with either methotrexate or
surgery
2. A 34-year-old G3P2012 presents with increased abdominal
C. Recheck the beta-hCG level in 1 week
girth and a history notable for tubal ligation 8 years previ-
D. Start the patient on an antibiotic regimen
ously. CT demonstrates a 23 × 14 × 26-cm, predominantly
cystic mass with thick internal septations, likely arising from 6. During pelvic examination of a 57-year-old woman, bilat-
the right ovary; and no ascites, lymphadenopathy, or addi- eral pelvic masses are palpated. Ultrasonography reveals
tional masses. Her CA-125 level is 28. Which one of the cystic and solid masses involving both ovaries. CT of the
following describes the appropriate next step? abdomen demonstrates an omental “cake.” Which one of
A. Pelvic ultrasonography the following tumor marker tests is indicated?
B. MRI A. Alpha-fetoprotein
C. Aspiration of cyst fluid for cytologic diagnosis B. CA-125
D. Exploratory laparotomy and removal of mass C. LDH
D. Beta-hCG
3. A 52-year-old, premenopausal woman presents to the emer-
gency department with pressure and pain. Ultrasonography 7. During pelvic examination of a 43-year-old G3P3, fullness is
reveals a complex, 10.7 × 15.9 × 8.5-cm mass on the left ovary. noted. Ultrasonography demonstrates bilateral tubular cyst-
Given the size of the mass, CT is performed, which confirms ic masses with short, round projections. Which one of the
the mass arising from the pelvis. No ascites, caking, or lym- following describes the appropriate next step?
phadenopathy is observed. The patient’s CA-125 level is 33.2 A. Immediate surgical excision
(laboratory normal <35). Which one of the following aspects in B. No further follow-up unless the patient becomes symp-
her history would prompt you to refer this patient to a gyneco- tomatic
logic oncologist? C. Evaluation of tumor marker levels
A. Mobile mass on examination D. Repeat ultrasonography in 1 year
B. History of prostate cancer in maternal grandfather
8. A 38-year-old G2P2 with a history of left salpingectomy pre-
C. Maternal history of breast cancer at age 40 years
sents to the emergency department with right lower abdom-
D. Paternal history of pancreatic cancer
inal pain, fever, spotting, and vomiting. She has no signifi-
4. During examination of a 34-year-old G2P2, a mass is pal- cant medical history, although a paternal aunt has premeno-
pated. A CA-125 level is obtained, and ultrasonography is pausal breast cancer. On examination, the patient is noted
performed. Ultrasonography reveals a simple, 2.8-cm, right to have cervical motion tenderness, and her white blood cell
ovarian cyst without nodularity or free fluid, but the patient’s count is 14.2. Ultrasonography demonstrates a 6 × 6.3 ×
CA-125 level is significantly elevated. Which one of the fol- 4-cm, complex, loculated, right adnexal mass with free fluid.
lowing is the least likely cause of this CA-125 elevation? Which one of the following describes the appropriate next
A. Pancreatic cancer step?
B. Endometriosis A. Diagnostic laparoscopy
C. Renal failure B. Treatment with antibiotics
D. Hepatic failure C. Repeat ultrasonography in 6 weeks
D. CA-125 level and CT scan
PGOv36n2.indd 7 12/18/15 4:06 PM
Topics in Obstetrics & Gynecology January 31, 2016
9. A 64-year-old G4P3013 with a history of hypertension pre- 10. A 36-year-old G0 presents for follow-up ultrasonography.
sents to the office with pelvic pressure and fullness. She is She moved from out of state and does not remember the
worried that she has cancer, but the discomfort is not sig- result of her prior ultrasonography, but she was told to have
nificant enough that she would want surgery. The remain- a repeat at some point. She is asymptomatic with mild, left-
der of this patient’s history is notable for tubal ligation at sided fullness on pelvic examination. Ultrasonography dem-
age 36 years and a sister with breast cancer diagnosed at onstrates a 6-cm mass with homogeneous, ground-glass
age 57 years. Pelvic examination demonstrates a small, echoes. Which of the following is the most likely diagnosis?
mobile uterus with fullness on the right. No discrete nodu- A. Corpus luteum cyst
larity is observed. Ultrasonography demonstrates a 5.5-cm B. Simple follicular cyst
simple right ovarian cyst—no free fluid and normal left C. Endometrioma
adnexa. Which one of the following describes the appropri- D. Ovarian neoplasm
ate next step?
A. Pelvic CT
B. Repeat ultrasonography in 12 months
C. Immediate surgical excision
D. Drainage to decrease size of the cyst
Dear Subscribers:
With this volume 36, we are pleased to introduce the new name of this newsletter: Topics in Obstetrics & Gynecology:
Practical CME Newsletter for Clinicians. We have changed the title to highlight the newsletter’s mission of providing
continuing medical education for practitioners who provide obstetric and gynecologic health care to women.
You will notice two other changes:
• The annual frequency of Topics in Obstetrics & Gynecology will be 18 issues (reduced from 24 issues).
• Each CME article will be designated for a maximum of 2.0 AMA PRA Category 1 Credits™, for the same annual total
of 36 CME credits that had been available previously.
Thank you for your continued support of this newsletter.
PGOv36n2.indd 8 12/18/15 4:06 PM
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Lefkowitz v. Great Minneapolis Surplus StoreDocument1 pageLefkowitz v. Great Minneapolis Surplus StorecrlstinaaaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Design of Reinforced Concrete Shear WallDocument8 pagesDesign of Reinforced Concrete Shear WallklynchelleNo ratings yet
- Algorithms For Big DataDocument458 pagesAlgorithms For Big DataAleksey KourbatovNo ratings yet
- A History of The Knights TemplarDocument79 pagesA History of The Knights TemplarСаша Рађеновић100% (3)
- Analisis Strategi Pembinaan Kesehatan Mental Oleh Guru Pengasuh Sekolah Berasrama Di Aceh Besar Pada Masa Pandemi Faisal Anwar & Putry JuliaDocument20 pagesAnalisis Strategi Pembinaan Kesehatan Mental Oleh Guru Pengasuh Sekolah Berasrama Di Aceh Besar Pada Masa Pandemi Faisal Anwar & Putry JuliaPutriNo ratings yet
- Arthur Peacocke - Creation and The World of Science - The Re-Shaping of Belief (2004)Document426 pagesArthur Peacocke - Creation and The World of Science - The Re-Shaping of Belief (2004)Nelson100% (3)
- Perdev Las2Document4 pagesPerdev Las2JoannNo ratings yet
- Bixler v. Scientology: Declaration of Margaret MarmolejoDocument86 pagesBixler v. Scientology: Declaration of Margaret MarmolejoTony OrtegaNo ratings yet
- Sample of Competency Framework in GEDocument34 pagesSample of Competency Framework in GEPareshNo ratings yet
- Booklist 2015-2016Document7 pagesBooklist 2015-2016Anonymous ysqtqPGUmQNo ratings yet
- Adopting Multifunctional Material SystemsDocument197 pagesAdopting Multifunctional Material Systems_AniMuS__No ratings yet
- IMO List of Recognized Test Laboratories October 2014 - tcm8-26040Document18 pagesIMO List of Recognized Test Laboratories October 2014 - tcm8-26040Kayhan AytuğNo ratings yet
- Unit 11: Things That Changed The WorldDocument50 pagesUnit 11: Things That Changed The Worldphonglantim3101No ratings yet
- The Effects of Digital StorytellingDocument12 pagesThe Effects of Digital StorytellingGuna SegarNo ratings yet
- The Construct of Resilience: Implications For Interventions and Social PoliciesDocument29 pagesThe Construct of Resilience: Implications For Interventions and Social PoliciesFeblin Follen Priscila SalindehoNo ratings yet
- Unit2Document22 pagesUnit2Sarah DewanNo ratings yet
- Ch. 3 Measuring Organizational EffectivenessDocument8 pagesCh. 3 Measuring Organizational EffectivenessDyahAyuRatnaCantikaNo ratings yet
- Applied Social Science: A Course IntroductionDocument36 pagesApplied Social Science: A Course IntroductionDennis RaymundoNo ratings yet
- Portraits As ObjectsDocument126 pagesPortraits As ObjectsWang HuaNo ratings yet
- Melchora AquinoDocument2 pagesMelchora AquinokylaNo ratings yet
- Radar PerformanceDocument30 pagesRadar PerformanceHarbinder Singh100% (3)
- Write Up On HUFDocument2 pagesWrite Up On HUFRajeshNo ratings yet
- Catharsis by Devapriya MukherjeeDocument9 pagesCatharsis by Devapriya MukherjeeCinnamonTeal PublishingNo ratings yet
- The Use of Korean Wave To Increase Global Korea Scholarship (GKS) Enthusiast To Promote South Korea Public Diplomacy in IndonesiaDocument8 pagesThe Use of Korean Wave To Increase Global Korea Scholarship (GKS) Enthusiast To Promote South Korea Public Diplomacy in Indonesiaamara prameswariNo ratings yet
- SONI - Fundamentals of Botany - Vol 2 (2011, MC GRAW HILL INDIA) PDFDocument398 pagesSONI - Fundamentals of Botany - Vol 2 (2011, MC GRAW HILL INDIA) PDFPrince Quokka Rai100% (5)
- Book Review: Physics of Radiology, 2nd Ed. by Anthony Brinton Wolbarst. Madison, WI: Medical Physics PublishingDocument1 pageBook Review: Physics of Radiology, 2nd Ed. by Anthony Brinton Wolbarst. Madison, WI: Medical Physics PublishingRoric ThomasNo ratings yet
- Chap 3 (1) - Problem SolvingDocument26 pagesChap 3 (1) - Problem SolvingEstifanosNo ratings yet
- TIM E Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDocument3 pagesTIM E Sunday Monday Tuesday Wednesday Thursday Friday SaturdayDàniéLewinskiNo ratings yet
- 106106126Document4 pages106106126Yeshwanth RangojuNo ratings yet
- MentalistDocument434 pagesMentalistAngeline ErcillaNo ratings yet