You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- AutoimmunediseasesDocument24 pagesAutoimmunediseasesCristina ZoițanuNo ratings yet
- Jagim2017 PDFDocument28 pagesJagim2017 PDFAnujGuptaNo ratings yet
- Tidy's Physiotherapy (15th Ed.) PDFDocument657 pagesTidy's Physiotherapy (15th Ed.) PDFTomas85% (53)
- Growthdisorder2 180323165227Document133 pagesGrowthdisorder2 180323165227AnujGuptaNo ratings yet
- JSSM 15 379Document8 pagesJSSM 15 379AnujGuptaNo ratings yet
- Mccrory 2017Document3 pagesMccrory 2017AnujGuptaNo ratings yet
- Jagim2017 PDFDocument28 pagesJagim2017 PDFAnujGuptaNo ratings yet
- Polrcari Elevation Training Mask JSSM2016Document9 pagesPolrcari Elevation Training Mask JSSM2016AnujGuptaNo ratings yet
- PNFDocument57 pagesPNFgialinu100% (3)
- Passive Mobilization Exercises Upper LimbDocument3 pagesPassive Mobilization Exercises Upper LimbAnujGuptaNo ratings yet
- 0Document32 pages0AnujGuptaNo ratings yet
- 5499chapter7Document34 pages5499chapter7AnujGuptaNo ratings yet
- Therapeutic Modalities ReviewDocument68 pagesTherapeutic Modalities ReviewAnujGuptaNo ratings yet
- Short Wave Diathermy: Sreeraj S RDocument31 pagesShort Wave Diathermy: Sreeraj S RAnujGuptaNo ratings yet
- Short Wave Diathermy: Sreeraj S RDocument31 pagesShort Wave Diathermy: Sreeraj S RAnujGuptaNo ratings yet
- Ch09 SWD FMTDocument15 pagesCh09 SWD FMTAnujGuptaNo ratings yet
- Anatomy Mnemonics Back LimbsDocument3 pagesAnatomy Mnemonics Back LimbsmarianadukNo ratings yet
- Ch09 SWD FMTDocument15 pagesCh09 SWD FMTAnujGuptaNo ratings yet
- Therapeutic Exercises: Fundamental and Derived PositionsDocument11 pagesTherapeutic Exercises: Fundamental and Derived PositionsAnujGuptaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Thing in Itself Kantian: AnstoßDocument1 pageThing in Itself Kantian: Anstoßwhynotbequiet23No ratings yet
- Manual Diagrama Detector de MetalesDocument18 pagesManual Diagrama Detector de MetalesEdmundo Cisneros0% (1)
- Is 800-2007 - Indian Code of Practice For Construction in SteelDocument41 pagesIs 800-2007 - Indian Code of Practice For Construction in SteelshiivendraNo ratings yet
- Appendix-Design CalculationsDocument3 pagesAppendix-Design CalculationsVanessa M. MartinezNo ratings yet
- Key Term Arabic Meaning Link: Life ScienceDocument5 pagesKey Term Arabic Meaning Link: Life ScienceReemNo ratings yet
- 1 Conformity Asch StudyDocument31 pages1 Conformity Asch StudyjasbruNo ratings yet
- DLL - English 5 - Q3 - W8Document8 pagesDLL - English 5 - Q3 - W8Merlyn S. Al-osNo ratings yet
- Option MCQ-Human Resource Management (205) : Clarifying Handling People Maintaing Relationship (C) Both (A) and (B)Document4 pagesOption MCQ-Human Resource Management (205) : Clarifying Handling People Maintaing Relationship (C) Both (A) and (B)MukulNo ratings yet
- One Word SubstitutionDocument5 pagesOne Word SubstitutionPranaykant Singh PanwarNo ratings yet
- Crystal Gallery: AccountabilityDocument15 pagesCrystal Gallery: AccountabilityJitesh ManwaniNo ratings yet
- 01-Toy Product DesignDocument54 pages01-Toy Product DesignJuanNo ratings yet
- Tssiig GC e Module 1 PDFDocument6 pagesTssiig GC e Module 1 PDFLoiweza AbagaNo ratings yet
- Swot Analysis of Revlon IncDocument5 pagesSwot Analysis of Revlon IncSubhana AsimNo ratings yet
- Title of The Training Program Regional Training of Grades 4-8 Reading Teachers On Care For Non-Readers (CNR) Program Module No., Day & Session NoDocument18 pagesTitle of The Training Program Regional Training of Grades 4-8 Reading Teachers On Care For Non-Readers (CNR) Program Module No., Day & Session Nomarvin susminaNo ratings yet
- Revise Chap 12Document14 pagesRevise Chap 12RACHEL DAMALERIONo ratings yet
- Pdlgfu15: PDLGFU15 User's GuideDocument327 pagesPdlgfu15: PDLGFU15 User's Guidejose antonio carazoNo ratings yet
- ApolloBVM PDFDocument41 pagesApolloBVM PDFShiva KumarNo ratings yet
- Evaluation - Chemical Pit - 0Document8 pagesEvaluation - Chemical Pit - 0Aiman AmirullahNo ratings yet
- Designing Research TopicDocument19 pagesDesigning Research TopicMark Padin VillaplazaNo ratings yet
- Intro Ducci OnDocument38 pagesIntro Ducci OnCARLOS EDUARDO AGUIRRE LEONNo ratings yet
- Worksheet - StatisticsDocument3 pagesWorksheet - StatisticsGabriel Ch MendezNo ratings yet
- Anti FoundationalismDocument4 pagesAnti FoundationalismKostasBaliotisNo ratings yet
- Alsabei ThesisDocument279 pagesAlsabei Thesisrayzo2182No ratings yet
- Summary Good To GreatDocument5 pagesSummary Good To GreatAziz ur RehmanNo ratings yet
- Belbin's Team ModelDocument2 pagesBelbin's Team Modelsonu_saisNo ratings yet
- FLIGHT Punta Arenas - SantiagoDocument3 pagesFLIGHT Punta Arenas - SantiagoАртем ПичугинNo ratings yet
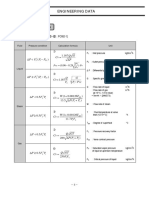
- Engineering Data: 2. CV CalculationDocument1 pageEngineering Data: 2. CV Calculationdj22500No ratings yet
- Assignment 1Document12 pagesAssignment 1Santosh SubramanyaNo ratings yet
- Healing GardensDocument7 pagesHealing GardensElvaNo ratings yet
- Upload Infotype 2006 (Absence Quotas) - Code Gallery - SCN WikiDocument3 pagesUpload Infotype 2006 (Absence Quotas) - Code Gallery - SCN WikiArun Varshney (MULAYAM)No ratings yet