You might also like
- Sample Discharge Summary TemplateDocument3 pagesSample Discharge Summary TemplateBobby Reddy100% (1)
- Discharge-Summary-Template JogiDocument1 pageDischarge-Summary-Template JogiJoginderNo ratings yet
- Dictation Discharge Summary TemplateDocument19 pagesDictation Discharge Summary TemplateBobby ReddyNo ratings yet
- Doctors NoteDocument6 pagesDoctors Noteitgivesyouwings9No ratings yet
- ToxicologyDocument2 pagesToxicologyTOD100% (1)
- Patient Summary - AWVDocument5 pagesPatient Summary - AWVAna FitzpatrickNo ratings yet
- Preoperative Risk Assessment / Clearance FormDocument1 pagePreoperative Risk Assessment / Clearance FormEster Lugo CapcoNo ratings yet
- Discharge Summary TemplateDocument1 pageDischarge Summary TemplateRinson JosephNo ratings yet
- Complete Blood Count Result Form Test Name Result Reference RangeDocument4 pagesComplete Blood Count Result Form Test Name Result Reference RangePau-pau BasiNo ratings yet
- 2 CA - Health Profile - 2014-12-19 PDFDocument9 pages2 CA - Health Profile - 2014-12-19 PDFLiamNo ratings yet
- Example Discharge Letters PDFDocument5 pagesExample Discharge Letters PDFlanghal100% (1)
- Vivitrol TreatmentDocument8 pagesVivitrol TreatmentHarish RathodNo ratings yet
- Ga TB Test Form OscarDocument1 pageGa TB Test Form OscarWilliamNo ratings yet
- Department of State Academic Exchanges Participant Medical History and Examination FormDocument8 pagesDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNo ratings yet
- Apostol - CTDocument4 pagesApostol - CTMarion Frances LagmayNo ratings yet
- Drug Dosing ChartDocument16 pagesDrug Dosing ChartdnaaziiNo ratings yet
- Consent For Release of Medical RecordsDocument1 pageConsent For Release of Medical RecordsCarrboro Family MedicineNo ratings yet
- Clear Form: Motor Vehicle Accident ReportDocument4 pagesClear Form: Motor Vehicle Accident ReportBodii BoftainNo ratings yet
- MN Res Home Energy Audit ReportDocument9 pagesMN Res Home Energy Audit ReportFarwa MalikNo ratings yet
- Detox OverviewDocument6 pagesDetox OverviewLauren ENo ratings yet
- Opioid Withdrawal ClinicalKeyDocument14 pagesOpioid Withdrawal ClinicalKeykuldip SinghNo ratings yet
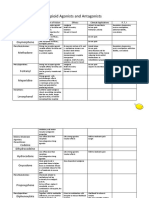
- Opioid Agonists and AntagonistsDocument5 pagesOpioid Agonists and AntagonistsCas BuNo ratings yet
- Combating The Opioid Crisis: The Department of Health and Human Services Must Update EMTALADocument21 pagesCombating The Opioid Crisis: The Department of Health and Human Services Must Update EMTALANew England Law ReviewNo ratings yet
- Admission LetterDocument18 pagesAdmission LetterBridget WardNo ratings yet
- Liverpool Outcome Score (LOS) For Assessing Adults at DischargeDocument3 pagesLiverpool Outcome Score (LOS) For Assessing Adults at Dischargekartika farahdillaNo ratings yet
- SUD I - Opioid-Related Disorders Cheat Sheet: by ViaDocument4 pagesSUD I - Opioid-Related Disorders Cheat Sheet: by ViaDonatella S.No ratings yet
- Vaccination Records - Children and TeensDocument4 pagesVaccination Records - Children and TeensverumluxNo ratings yet
- Initial Hospital Visit Inpatient Consult NoteDocument6 pagesInitial Hospital Visit Inpatient Consult NoteJanu easwarNo ratings yet
- New Patient FormDocument7 pagesNew Patient Forme-MedTools100% (4)
- Ham ADocument1 pageHam Araj1969No ratings yet
- Medical Record of PetsDocument24 pagesMedical Record of PetsMari AguilarNo ratings yet
- Subutex Quick-Start-GuideDocument6 pagesSubutex Quick-Start-GuideDanNo ratings yet
- Gynae Care Plan ECTOPIC ReviewedDocument2 pagesGynae Care Plan ECTOPIC ReviewedDet LaurenteNo ratings yet
- Patient Details Date: Ref No: Address: PH No.:: Dr. Vanisha Mattu MbbsDocument1 pagePatient Details Date: Ref No: Address: PH No.:: Dr. Vanisha Mattu MbbsrksjprNo ratings yet
- Covid Test 3Document1 pageCovid Test 3Marius MateiNo ratings yet
- Species DiagnosesDocument33 pagesSpecies DiagnosesJoanneYiNo ratings yet
- Policy Vaccination Record CardDocument2 pagesPolicy Vaccination Record CardGurpreetNo ratings yet
- SITEL - Claims Reimbursement Form Rev.06 PDFDocument2 pagesSITEL - Claims Reimbursement Form Rev.06 PDFJoyce HerreraNo ratings yet
- Skin Rashes Guideline in Paediatric Emergency Department (Cross Site)Document33 pagesSkin Rashes Guideline in Paediatric Emergency Department (Cross Site)Eskilda LucildaNo ratings yet
- Ontario - Schedule of Benefits 2021Document970 pagesOntario - Schedule of Benefits 2021Raj LoganathanNo ratings yet
- SpirochetesDocument30 pagesSpirochetesDaniel AtiehNo ratings yet
- Varicella ZosterDocument41 pagesVaricella Zostertummalapalli venkateswara raoNo ratings yet
- Mark Amundsen 3-12-13 UCDavis Med CTRDocument2,608 pagesMark Amundsen 3-12-13 UCDavis Med CTRSarah OlsonNo ratings yet
- Cuny Immunization Record FormDocument2 pagesCuny Immunization Record Formmichael JacksonNo ratings yet
- Medicina InternaDocument1,239 pagesMedicina Internaandres felipe75% (4)
- Immunization RecordDocument1 pageImmunization RecordJane PhamNo ratings yet
- What Makes A TeamDocument3 pagesWhat Makes A TeamGretel BanosNo ratings yet
- Josephine Ball ResumeDocument1 pageJosephine Ball Resumeapi-483700218No ratings yet
- Strep Throat FactsDocument2 pagesStrep Throat FactsFactPaloozaNo ratings yet
- Walgreen's Vaccination FormDocument2 pagesWalgreen's Vaccination Formcarina811No ratings yet
- Output PDFDocument3 pagesOutput PDFTrunali GabhaneNo ratings yet
- Immunology Spe Dual Marker: 10553470 Mrs - Ananya MishraDocument3 pagesImmunology Spe Dual Marker: 10553470 Mrs - Ananya MishraÑîrañjañ JhåNo ratings yet
- Taboso, Glory Jane Bonina 2086021045Document1 pageTaboso, Glory Jane Bonina 2086021045Jane Bornasal BoninaNo ratings yet
- Ekg Cheat SheetDocument5 pagesEkg Cheat SheetAnonymous QBa0UurPNo ratings yet
- Safe Methadone Induction and Stabilization Report-1 PDFDocument10 pagesSafe Methadone Induction and Stabilization Report-1 PDFDel Rio LauraNo ratings yet
- Name: - Age: - Sex: - AddressDocument1 pageName: - Age: - Sex: - AddresskNo ratings yet
- De1101id PDFDocument12 pagesDe1101id PDFEvette M. SolteszNo ratings yet
- Nurse Practitioner Wound Management Clinical ProtocolsDocument29 pagesNurse Practitioner Wound Management Clinical ProtocolsBrian HarrisNo ratings yet
- Janumet-Xr MakassarDocument49 pagesJanumet-Xr MakassarSuardy CiayadiNo ratings yet
- Pharmacologic Treatment of OpioidDocument17 pagesPharmacologic Treatment of OpioidWHYY NewsNo ratings yet
- EKG+Mastery +ischemiaDocument6 pagesEKG+Mastery +ischemiamoussa medjahedNo ratings yet
- Negative: What Does It Mean To Have A Test Result?Document1 pageNegative: What Does It Mean To Have A Test Result?Kyle SchroederNo ratings yet
- Prescription Template 07Document2 pagesPrescription Template 07vincent100% (1)
- 耶鲁大学 免疫表格immunization Form 2021-7-30Document2 pages耶鲁大学 免疫表格immunization Form 2021-7-30Chris HahaNo ratings yet
- NSU Housing - Immunizations 2021Document2 pagesNSU Housing - Immunizations 2021rcastacNo ratings yet
- Vagus Indigestion in Bovines: A Review in Historical PerspectiveDocument8 pagesVagus Indigestion in Bovines: A Review in Historical PerspectiveSara ConnorNo ratings yet
- HerpesDocument2 pagesHerpesSyafruddin GBNo ratings yet
- Common Flu and ColdDocument8 pagesCommon Flu and ColdАнгелина ПрибыльскаяNo ratings yet
- Veterinarian: By: Aubrynn BakerDocument11 pagesVeterinarian: By: Aubrynn BakeraubrynnNo ratings yet
- Dean Director Post AdvtDocument14 pagesDean Director Post AdvtSingh BhujangiNo ratings yet
- Vaccines Reading ComprehensionDocument2 pagesVaccines Reading ComprehensionYolanda RamonNo ratings yet
- Filarial Worms AssignmentDocument3 pagesFilarial Worms AssignmentNokuthaba SiyafaNo ratings yet
- Amputation of Tail in Buff JournalDocument9 pagesAmputation of Tail in Buff JournalKhawaja usmanNo ratings yet
- Infectious DiseasesDocument96 pagesInfectious DiseasesSuvasish SuvasishNo ratings yet
- California School Immunization RecordDocument2 pagesCalifornia School Immunization RecordJeevitha RoyapathiNo ratings yet
- Humoral Immune ResponseDocument22 pagesHumoral Immune ResponseAlunaficha Melody KiraniaNo ratings yet
- Whooping Cough (Pertussis) InformationDocument2 pagesWhooping Cough (Pertussis) InformationtombstoneepitaphNo ratings yet
- Latent TBDocument24 pagesLatent TBLouis FortunatoNo ratings yet
- Manual On Meat Inspection For Developing CountriesDocument335 pagesManual On Meat Inspection For Developing CountriesRoxana Elena M0% (1)
- Sinus Infection (Sinusitis) in ChickensDocument6 pagesSinus Infection (Sinusitis) in ChickensShah NawazNo ratings yet
- Table - Diseases Notifiable To The OIEDocument1 pageTable - Diseases Notifiable To The OIEЂорђе100% (1)
- Chain of InfectionDocument2 pagesChain of Infectionapi-251976647No ratings yet
- Revisi - Pathophysiology and Pathogenesis Covid 19 - FELIX KHOSASIDocument29 pagesRevisi - Pathophysiology and Pathogenesis Covid 19 - FELIX KHOSASIfelixNo ratings yet
- Human Blood GroupsDocument29 pagesHuman Blood GroupsKunalNo ratings yet
- Classification SL - No Disease Rickettsial Agent Insect Vector Mammalian ReservoirsDocument4 pagesClassification SL - No Disease Rickettsial Agent Insect Vector Mammalian ReservoirsGetom NgukirNo ratings yet
- Veterinary Professional Ethics TSDocument12 pagesVeterinary Professional Ethics TSKrešimir SeverinNo ratings yet
- Animal Welfare, Animal RightsDocument8 pagesAnimal Welfare, Animal RightsDevynNo ratings yet
- Citation of Professor Morenike DipeoluDocument23 pagesCitation of Professor Morenike DipeoluAkinola Oluwatoyin CharlesNo ratings yet
- Gahp Standard Malaysia Final DraftedDocument25 pagesGahp Standard Malaysia Final DraftedFcpo Bursa Malaysia100% (1)