You might also like
- Navigating Long-Term Care - A Practical Approach for NursesFrom EverandNavigating Long-Term Care - A Practical Approach for NursesNo ratings yet
- Textbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersFrom EverandTextbook of Urgent Care Management: Chapter 34, Engaging Accountable Care Organizations in Urgent Care CentersNo ratings yet
- NURSING THE CHILDBEARING FAMILY: Passbooks Study GuideFrom EverandNURSING THE CHILDBEARING FAMILY: Passbooks Study GuideNo ratings yet
- Healthcare Environmental Services A Complete Guide - 2020 EditionFrom EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNo ratings yet
- Utilization Review Coordinator: Passbooks Study GuideFrom EverandUtilization Review Coordinator: Passbooks Study GuideNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- The Nurse Practitioner in UrologyFrom EverandThe Nurse Practitioner in UrologyMichelle LajinessNo ratings yet
- Supervising Registered Nurse: Passbooks Study GuideFrom EverandSupervising Registered Nurse: Passbooks Study GuideNo ratings yet
- NURSING ADMINISTRATION: Passbooks Study GuideFrom EverandNURSING ADMINISTRATION: Passbooks Study GuideNo ratings yet
- Managing Diabetes and Hyperglycemia in the Hospital Setting: A Clinician's GuideFrom EverandManaging Diabetes and Hyperglycemia in the Hospital Setting: A Clinician's GuideNo ratings yet
- Addiction in the Lives of Registered Nurses and Their Wake-Up Jolt to RecoveryFrom EverandAddiction in the Lives of Registered Nurses and Their Wake-Up Jolt to RecoveryNo ratings yet
- A few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentFrom EverandA few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentNo ratings yet
- Your Health, Your Decisions: How to Work with Your Doctor to Become a Knowledge-Powered PatientFrom EverandYour Health, Your Decisions: How to Work with Your Doctor to Become a Knowledge-Powered PatientNo ratings yet
- Board Certified Nurse Practitioner in Savannah GA Resume Michele StephensDocument4 pagesBoard Certified Nurse Practitioner in Savannah GA Resume Michele StephensMicheleStephens100% (1)
- Textbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipFrom EverandTextbook of Urgent Care Management: Chapter 24, Revenue Cycle Management and PartnershipNo ratings yet
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeFrom EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeNo ratings yet
- Professional ResumeDocument1 pageProfessional ResumeDouglas RutledgeNo ratings yet
- Pharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsFrom EverandPharmacotherapeutic Management of Cardiovascular Disease Complications: A Textbook for Medical StudentsNo ratings yet
- Textbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineFrom EverandTextbook of Urgent Care Management: Chapter 33, EMTALA in Urgent Care MedicineNo ratings yet
- Department of Transportation Medical Reference for ExaminersFrom EverandDepartment of Transportation Medical Reference for ExaminersNo ratings yet
- Diabetes Management in Long-Term Settings: A Clinician's Guide to Optimal Care for the ElderlyFrom EverandDiabetes Management in Long-Term Settings: A Clinician's Guide to Optimal Care for the ElderlyNo ratings yet
- Care Coordination And Management Applications A Complete Guide - 2020 EditionFrom EverandCare Coordination And Management Applications A Complete Guide - 2020 EditionNo ratings yet
- Clinical Cases in Right Heart FailureFrom EverandClinical Cases in Right Heart FailureLana TsaoNo ratings yet
- Textbook of Urgent Care Management: Chapter 20, Strategic Talent Management: Talent Makes All the DifferenceFrom EverandTextbook of Urgent Care Management: Chapter 20, Strategic Talent Management: Talent Makes All the DifferenceNo ratings yet
- How to Maximize Your Time and Minimize Your Stress in HealthcareFrom EverandHow to Maximize Your Time and Minimize Your Stress in HealthcareNo ratings yet
- NURSING ADMINISTRATION, ADVANCED: Passbooks Study GuideFrom EverandNURSING ADMINISTRATION, ADVANCED: Passbooks Study GuideNo ratings yet
- Certified Laboratory Assistant: Passbooks Study GuideFrom EverandCertified Laboratory Assistant: Passbooks Study GuideNo ratings yet
- Are Your Meds Making You Sick?: A Pharmacist's Guide to Avoiding Dangerous Drug Interactions, Reactions, and Side-EffectsFrom EverandAre Your Meds Making You Sick?: A Pharmacist's Guide to Avoiding Dangerous Drug Interactions, Reactions, and Side-EffectsNo ratings yet
- Textbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordFrom EverandTextbook of Urgent Care Management: Chapter 23, Choosing the Electronic Health RecordNo ratings yet
- Necrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNecrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Clinical Guidelines and Care ProtocolsFrom EverandClinical Guidelines and Care ProtocolsRating: 5 out of 5 stars5/5 (1)
- Registered Professional Nurse: Passbooks Study GuideFrom EverandRegistered Professional Nurse: Passbooks Study GuideNo ratings yet
- Hospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsFrom EverandHospitalist Program Toolkit: A Comprehensive Guide to Implementation of Successful Hospitalist ProgramsNo ratings yet
- Critical Care Nutrition Therapy for Non-nutritionistsFrom EverandCritical Care Nutrition Therapy for Non-nutritionistsMette M. BergerNo ratings yet
- Textbook of Urgent Care Management: Chapter 2, Developing a Business PlanFrom EverandTextbook of Urgent Care Management: Chapter 2, Developing a Business PlanNo ratings yet
- Health Information Technology A Complete Guide - 2020 EditionFrom EverandHealth Information Technology A Complete Guide - 2020 EditionNo ratings yet
- Psychiatry Practice BoostersFrom EverandPsychiatry Practice BoostersJesse KoskeyNo ratings yet
- House Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldFrom EverandHouse Calls 101: The Complete Clinician's Guide To In-Home Health Care, Telemedicine Services, and Long-Distance Treatment For a Post-Pandemic WorldNo ratings yet
- Understanding Your Child's and Teen's Behavior: Simple Steps and Resources to Guide You Through the JourneyFrom EverandUnderstanding Your Child's and Teen's Behavior: Simple Steps and Resources to Guide You Through the JourneyNo ratings yet
- Preoperative Risk Assessment / Clearance FormDocument1 pagePreoperative Risk Assessment / Clearance FormEster Lugo CapcoNo ratings yet
- Fluid Electrolyte TherapyDocument15 pagesFluid Electrolyte Therapyaarm1990No ratings yet
- Surgical Clearance FormDocument1 pageSurgical Clearance FormEster Lugo CapcoNo ratings yet
- Preoperative Risk Assessment / Clearance FormDocument1 pagePreoperative Risk Assessment / Clearance FormEster Lugo CapcoNo ratings yet
- Please Wear Face Mask and Face Shield - Google SearchDocument1 pagePlease Wear Face Mask and Face Shield - Google SearchEster Lugo CapcoNo ratings yet
- Permissive HypotensionDocument7 pagesPermissive HypotensionAdhytya Pratama AhmadiNo ratings yet
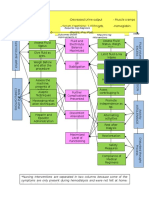
- Critical Care Concept Map 2Document1 pageCritical Care Concept Map 2nursing concept mapsNo ratings yet
- Syncope - Approach To The Patient Dynamed 2020 PDFDocument76 pagesSyncope - Approach To The Patient Dynamed 2020 PDFHeriberto Moreno HernandezNo ratings yet
- Mobile Blood DonationDocument10 pagesMobile Blood DonationChristine ApoloNo ratings yet
- PAL: Histology Connective Tissue Quiz Question 1Document20 pagesPAL: Histology Connective Tissue Quiz Question 1muryum100% (1)
- Hydatidiform MoleDocument2 pagesHydatidiform MolePaola AgustinNo ratings yet
- ChecklistDocument4 pagesChecklistRysan100% (1)
- PN NCLEX PRACTICE TESTDocument75 pagesPN NCLEX PRACTICE TESTjedisay1100% (1)
- 19 AD CBT Mock Questions A4 V1 PDFDocument29 pages19 AD CBT Mock Questions A4 V1 PDFAncy JustineNo ratings yet
- Anemia - Ferrum MetDocument6 pagesAnemia - Ferrum MetManali JainNo ratings yet
- Andrew Solomon Case Study - EditedDocument5 pagesAndrew Solomon Case Study - EditedJefferson KagiriNo ratings yet
- Management of Alveolar Ridge ResorptionDocument29 pagesManagement of Alveolar Ridge Resorptionفواز نميرNo ratings yet
- UH Neurosurgery Tips: Presenting on RoundsDocument2 pagesUH Neurosurgery Tips: Presenting on RoundsAndré PérezNo ratings yet
- Surgically Assisted Rapid Palatal Expansion: A Literature ReviewDocument13 pagesSurgically Assisted Rapid Palatal Expansion: A Literature ReviewjoserodrrNo ratings yet
- Early clinical exposure in the Neonatology unitDocument17 pagesEarly clinical exposure in the Neonatology unitPentolNo ratings yet
- Active and Passive ImmunizationDocument11 pagesActive and Passive ImmunizationNgakanNo ratings yet
- BLS MCQDocument22 pagesBLS MCQGeraldine Augusta100% (1)
- Medical AbbreviationDocument13 pagesMedical AbbreviationRaf Luis100% (1)
- COVID-19 Infodemic Study Analyzes Virus Naming and Social ContagionDocument10 pagesCOVID-19 Infodemic Study Analyzes Virus Naming and Social Contagionvivitri.dewiNo ratings yet
- Sign 108Document108 pagesSign 108Fibrianti Ratna SariNo ratings yet
- Hematology Review Section on Blood Cells and DevelopmentDocument79 pagesHematology Review Section on Blood Cells and DevelopmentLUZVIMINDA GORDONo ratings yet
- Current Surgical Therapy 13th EditionDocument61 pagesCurrent Surgical Therapy 13th Editiongreg.vasquez490100% (40)
- A Case Presentation of Diabetes Mellitus Type 2 Uncontrolled Non-Healing WoundDocument47 pagesA Case Presentation of Diabetes Mellitus Type 2 Uncontrolled Non-Healing Woundashamy acolNo ratings yet
- Icpc Pembahasan Coding Dengan IcpcDocument52 pagesIcpc Pembahasan Coding Dengan IcpcMelita RamadhaniNo ratings yet
- Cardio SLE Mcqs With AnswersDocument37 pagesCardio SLE Mcqs With AnswersAsif Newaz100% (4)
- Mycology Report 2Document6 pagesMycology Report 2Ange OuedraogoNo ratings yet
- Autism Symptoms ChecklistDocument1 pageAutism Symptoms ChecklistkarunaNo ratings yet
- ColposDocument41 pagesColposjumgzb 10No ratings yet
- Assessment 011 1Document12 pagesAssessment 011 1ManawNo ratings yet
- Dengue (Break Bone Fever) - FAQ, DPH-TAMIL NADU, IndiaDocument3 pagesDengue (Break Bone Fever) - FAQ, DPH-TAMIL NADU, IndiaDr.SagindarNo ratings yet