You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 1 CathDocument12 pages1 CathHashem AlsmadiNo ratings yet
- 300+ TOP RADIOLOGY Objective Questions and AnswersDocument26 pages300+ TOP RADIOLOGY Objective Questions and Answersمحمد سلمان100% (1)
- Assessment, Controversy, and Confounding Factors: Brain DeathDocument23 pagesAssessment, Controversy, and Confounding Factors: Brain DeathdewiNo ratings yet
- Carl Zeiss FF 450 - en - 07.10.1996Document50 pagesCarl Zeiss FF 450 - en - 07.10.1996Manuel FloresNo ratings yet
- CardionotesDocument5 pagesCardionotesNichole Coletta100% (1)
- Spesifikasi Allura XPER FD 20 (Clarity IQ)Document3 pagesSpesifikasi Allura XPER FD 20 (Clarity IQ)Yustina Lita SariNo ratings yet
- Journal Reading Radiologi EllaDocument44 pagesJournal Reading Radiologi EllaElla Putri SaptariNo ratings yet
- 2137 FullDocument7 pages2137 FullCourtneykdNo ratings yet
- DNB Systemwise Questions Customized (Space For Notes) Upto Dec 2019 PDFDocument252 pagesDNB Systemwise Questions Customized (Space For Notes) Upto Dec 2019 PDFGovindNo ratings yet
- Ci Content SpecificationsDocument6 pagesCi Content SpecificationsRoric ThomasNo ratings yet
- Cavernous Hemangioma of Mandible: A Rare Case ReportDocument5 pagesCavernous Hemangioma of Mandible: A Rare Case ReportAna CernaianuNo ratings yet
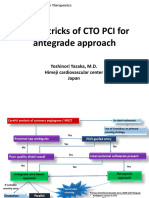
- Tips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanDocument21 pagesTips & Tricks of CTO PCI For Antegrade Approach: Yoshinori Yasaka, M.D. Himeji Cardiovascular Center JapanEll KlazureNo ratings yet
- T3 - Pack Code DetailsDocument302 pagesT3 - Pack Code DetailskiranNo ratings yet
- Lesson 4Document3 pagesLesson 4NER CARLO SANTOSNo ratings yet
- What Is A Brain AVMDocument5 pagesWhat Is A Brain AVMCj UritaNo ratings yet
- CardiologiaDocument36 pagesCardiologiaJulián Eduardo MorenoNo ratings yet
- Angina Pectoris PathophysiologyDocument12 pagesAngina Pectoris PathophysiologyJoyce Ann ArenasNo ratings yet
- Assessment and Impact of The Human Coronary CollateralDocument10 pagesAssessment and Impact of The Human Coronary CollateralSitiMaghfirahHafizNo ratings yet
- Is Iso 10555 2 1996Document14 pagesIs Iso 10555 2 1996Hemant SharmaNo ratings yet
- Bootcamp 1 CTA Techniques - MitsumoriDocument72 pagesBootcamp 1 CTA Techniques - MitsumorirmdeloneyNo ratings yet
- Neuroimaging in Acute StrokeDocument23 pagesNeuroimaging in Acute StrokeSnezana Mihajlovic100% (1)
- Carotid Artery Disease: Causes, Symptoms, Tests, and TreatmentDocument6 pagesCarotid Artery Disease: Causes, Symptoms, Tests, and TreatmentVijay Baskar SNo ratings yet
- How I Bypassed My Bypass-SurgeryDocument4 pagesHow I Bypassed My Bypass-Surgeryharinag49No ratings yet
- Avanta Fluid ManagementDocument108 pagesAvanta Fluid ManagementmonazzhNo ratings yet
- 50 Imaging Studies Every Doctor Should KnowDocument353 pages50 Imaging Studies Every Doctor Should KnowBaebee LouNo ratings yet
- Junsay, Twinkle Mae D. Section A - Group 10 History #1Document15 pagesJunsay, Twinkle Mae D. Section A - Group 10 History #1Twinkle Mae JunsayNo ratings yet
- C Memberaccess PDF Iqor BrochureDocument12 pagesC Memberaccess PDF Iqor BrochureJoanna MariketNo ratings yet
- Onyx Liquid Embolic System Coding Reimbursement GuideDocument8 pagesOnyx Liquid Embolic System Coding Reimbursement GuideronnyNo ratings yet
- Editor's Choice-How To Use D-Dimer in Acute Cardiovascular CareDocument12 pagesEditor's Choice-How To Use D-Dimer in Acute Cardiovascular Carefajar jamaloedinzNo ratings yet
- Non Contrast MRA 1Document39 pagesNon Contrast MRA 1ChriswinNo ratings yet