You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Language and Society-Research ProposalDocument8 pagesLanguage and Society-Research Proposalp3tru_mzq100% (2)
- Science F1 - Cell As A Unit of LifeDocument8 pagesScience F1 - Cell As A Unit of LifeamyryuzainiNo ratings yet
- PleureziileDocument18 pagesPleureziilep3tru_mzqNo ratings yet
- Chest X-Rays PDFDocument39 pagesChest X-Rays PDFp3tru_mzqNo ratings yet
- 19.inc. FrontosuboccDocument1 page19.inc. Frontosuboccp3tru_mzqNo ratings yet
- Non Canonical American WritersDocument4 pagesNon Canonical American Writersp3tru_mzqNo ratings yet
- Ralph Waldo EmersonDocument7 pagesRalph Waldo Emersonp3tru_mzqNo ratings yet
- Social ClassDocument2 pagesSocial Classp3tru_mzq100% (1)
- The Reporter's FunctionDocument3 pagesThe Reporter's Functionp3tru_mzqNo ratings yet
- Meat Lab Ex. 1Document15 pagesMeat Lab Ex. 1Emerlinda OlivaNo ratings yet
- Access N PMTCTDocument21 pagesAccess N PMTCTByaruhanga EmmanuelNo ratings yet
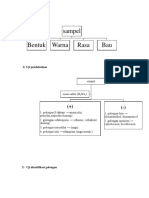
- Sampel Bentuk Warna Rasa Bau: 1) Uji OrganoleptikDocument3 pagesSampel Bentuk Warna Rasa Bau: 1) Uji OrganoleptikDinda AmandaNo ratings yet
- Transfusi: Ristiawan Muji Laksono Lab/Smf Anestesi Dan Terapi Intensif Fkub-RssaDocument34 pagesTransfusi: Ristiawan Muji Laksono Lab/Smf Anestesi Dan Terapi Intensif Fkub-RssaBryand KostaNo ratings yet
- Charateristics of NewbornDocument3 pagesCharateristics of NewbornRagupathyRamanjuluNo ratings yet
- EPI Manual For BHS 2017Document344 pagesEPI Manual For BHS 2017samuel winphyoeNo ratings yet
- Gerd - NCCP - Kppik 2011 (Hotel Shangri La)Document28 pagesGerd - NCCP - Kppik 2011 (Hotel Shangri La)Fatmala HaningtyasNo ratings yet
- Problems & Prospects of Dairy Milk Industry of Bidar DistrictDocument6 pagesProblems & Prospects of Dairy Milk Industry of Bidar DistrictnaveenNo ratings yet
- Muscles of MasticationDocument8 pagesMuscles of MasticationNaisi Naseem100% (1)
- Dka and HonkDocument30 pagesDka and HonkignasachyntiaNo ratings yet
- ScabiesDocument2 pagesScabiesPRINTDESK by DanNo ratings yet
- Referat Asma Pada AnakDocument18 pagesReferat Asma Pada AnakezuherliNo ratings yet
- Lecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesDocument58 pagesLecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesJharaNo ratings yet
- Harold Hemenway Are The Food Laws Scientific?Document44 pagesHarold Hemenway Are The Food Laws Scientific?thetruththewholetruthandnothingbutthetruth100% (4)
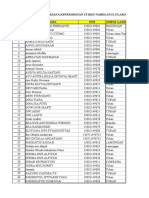
- Data Wisudawan Sarjana KeperawatanDocument15 pagesData Wisudawan Sarjana KeperawatanKhoridatuz Zuhriyah100% (1)
- Anatomy and Physiology of The Respiratory SystemDocument3 pagesAnatomy and Physiology of The Respiratory SystemLyka100% (1)
- Clinical Report July 6th 2017Document34 pagesClinical Report July 6th 2017ilhammandalaNo ratings yet
- Human Biology Concepts and Current Issues 8th Edition Johnson Test Bank DownloadDocument31 pagesHuman Biology Concepts and Current Issues 8th Edition Johnson Test Bank DownloadJustin Hunter100% (35)
- About Pink DolphinDocument12 pagesAbout Pink DolphinRiswan Hanafyah HarahapNo ratings yet
- KISA Biology QPDocument8 pagesKISA Biology QPakif.saitNo ratings yet
- 19.excretory Products and Their EliminationDocument21 pages19.excretory Products and Their Eliminationg1307No ratings yet
- Acute Exudative TonsillitisDocument4 pagesAcute Exudative TonsillitisRiska PashaNo ratings yet
- Anatomy and Physiology of Female Reproductive SystemDocument6 pagesAnatomy and Physiology of Female Reproductive SystemFarlyn Real MoralesNo ratings yet
- Phimosis N ParaphimosisDocument14 pagesPhimosis N ParaphimosisDhella 'gungeyha' RangkutyNo ratings yet
- Histology Practical PDF Bytom CnaanDocument65 pagesHistology Practical PDF Bytom CnaanMichel MunozNo ratings yet
- Human Body Systems Unit-8 6404 Ppt-1Document53 pagesHuman Body Systems Unit-8 6404 Ppt-1chohan artsNo ratings yet
- Banish Hives Forever EbookDocument29 pagesBanish Hives Forever EbookSarah BayaNo ratings yet
- Salivary Secretion: Chapter OutlineDocument9 pagesSalivary Secretion: Chapter OutlineJoshika MahendranNo ratings yet
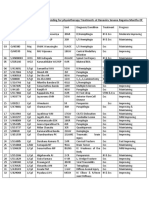
- Progress Report of Indoor Patients Attending For Physiotherapy Treatment atDocument6 pagesProgress Report of Indoor Patients Attending For Physiotherapy Treatment atIsuru DasanthaNo ratings yet