You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
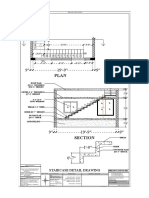
- Staircase Detail Drawing: Roof Slab @0'-6" TJICKNESS @10'-0" HEIGHTDocument1 pageStaircase Detail Drawing: Roof Slab @0'-6" TJICKNESS @10'-0" HEIGHTDhineshNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 300+ TOP ESTIMATING & COSTING Multiple Choice Questions AnswersDocument39 pages300+ TOP ESTIMATING & COSTING Multiple Choice Questions AnswersDhineshNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- RVS School of Architecture, DindigulDocument5 pagesRVS School of Architecture, DindigulDhineshNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Urban DesignDocument11 pagesUrban DesignDhineshNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 01.unit 1 - Specification & Specification WritingDocument26 pages01.unit 1 - Specification & Specification WritingDhineshNo ratings yet
- Paper With Solutions PDFDocument40 pagesPaper With Solutions PDFDhineshNo ratings yet
- Presentation1 160229160253 PDFDocument50 pagesPresentation1 160229160253 PDFDhinesh100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- House Rules - Melton Study Report and RecommendationsDocument90 pagesHouse Rules - Melton Study Report and RecommendationsDhineshNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Free Download Time Saver Standards Architectural Design BookDocument3 pagesFree Download Time Saver Standards Architectural Design BookDhinesh50% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Executive SummaryDocument39 pagesExecutive Summarytanisq10No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Sasi MeDocument32 pagesSasi MeDINUNo ratings yet
- Group 2 - Sec F PhonePe PDFDocument20 pagesGroup 2 - Sec F PhonePe PDFMaitresh Agarwal0% (1)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- NUENO QUELCH - Mass Marketing of LuxuryDocument8 pagesNUENO QUELCH - Mass Marketing of LuxuryElita H.No ratings yet
- Quantitative ResearchDocument56 pagesQuantitative ResearchMaksen LimNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Digital Marketing BasicsDocument52 pagesDigital Marketing BasicsWe strategist100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Service MarketingDocument11 pagesService Marketinggaurav bhardwajNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Report On DARAZ Bangladesh Prepared ForDocument31 pagesReport On DARAZ Bangladesh Prepared ForFarhanur RahmanNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- LG Balancing Urban& Rural SegmentDocument29 pagesLG Balancing Urban& Rural SegmentRiyas NoorudeenNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Swot Analysis of Lenovo by Kamal Kant Soni at Pg-08-36Document9 pagesSwot Analysis of Lenovo by Kamal Kant Soni at Pg-08-36Kamal Soni100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Millionare Real Estate GuideDocument12 pagesThe Millionare Real Estate GuideJose Antonio Vasquez100% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- WHAT IS ADVERTISING - SlidesDocument17 pagesWHAT IS ADVERTISING - Slideschristina kawihingNo ratings yet
- Apple Marketing PlanDocument33 pagesApple Marketing PlanGuru Katz100% (2)
- Advanced Performance Management: Thursday 4 June 2015Document13 pagesAdvanced Performance Management: Thursday 4 June 2015Tiffany ToonNo ratings yet
- Blockerdiondra Resume2Document1 pageBlockerdiondra Resume2api-526836825No ratings yet
- Supply Chain ManagmentDocument4 pagesSupply Chain ManagmentNeel Shyam Tyagi0% (1)
- SM CaseDocument13 pagesSM CaseFatema SultanaNo ratings yet
- Part IDocument51 pagesPart IDanielNo ratings yet
- B2BM Case Maersk LineDocument23 pagesB2BM Case Maersk LineRoshan GurjarNo ratings yet
- CRM Process: Submitted byDocument15 pagesCRM Process: Submitted bySwati JaretNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- ELTU2012 - 3b - Business Proposals Structure (Student Version) August 2017 (1) - 1Document20 pagesELTU2012 - 3b - Business Proposals Structure (Student Version) August 2017 (1) - 1Donald TangNo ratings yet
- Marketing Strategies For Fast-Food Restaurants: A Customer ViewDocument7 pagesMarketing Strategies For Fast-Food Restaurants: A Customer ViewabhishekmonNo ratings yet
- Ecourier News FTDocument1 pageEcourier News FTGiacomo GiovannoneNo ratings yet
- Case Study Analysis On Baxton TechnologyDocument2 pagesCase Study Analysis On Baxton TechnologyThamarai SelviNo ratings yet
- 1 QuizDocument23 pages1 QuizThu Hiền KhươngNo ratings yet
- 114, Prakash Purohit, MicromaxDocument21 pages114, Prakash Purohit, MicromaxKhan AlamNo ratings yet
- A Study On Customer Satisfaction With Reference To Amazon Online ShoppingDocument20 pagesA Study On Customer Satisfaction With Reference To Amazon Online Shoppingjeel rabadiya60% (5)
- Unilever CaseDocument4 pagesUnilever Caserhaecal100% (1)
- EXSERVS Mariwasa Case 2Document2 pagesEXSERVS Mariwasa Case 2Lui CastañedaNo ratings yet
- Marketing Mix by DjKatyDocument30 pagesMarketing Mix by DjKatykysecempeNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)