You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Assessment Diagnosis Planning Implementation EvaluationDocument3 pagesAssessment Diagnosis Planning Implementation EvaluationIvy Villalobos100% (1)
- Nose Picking Relative Humidity Respiratory Tract Infections Chronic Sinusitis Rhinitis IrritantsDocument2 pagesNose Picking Relative Humidity Respiratory Tract Infections Chronic Sinusitis Rhinitis Irritantslourdes kusumadiNo ratings yet
- Factors Influencing The Implementation of Global Polio Eradication Initiative in Low and Middle Income Countries A Qualitative Evidence SynthesisDocument12 pagesFactors Influencing The Implementation of Global Polio Eradication Initiative in Low and Middle Income Countries A Qualitative Evidence Synthesislourdes kusumadiNo ratings yet
- Lo Hemato Week 3Document4 pagesLo Hemato Week 3lourdes kusumadiNo ratings yet
- Absorbance Concentration 0,12 50 0,148 100 0,125 150 0,152 200Document2 pagesAbsorbance Concentration 0,12 50 0,148 100 0,125 150 0,152 200lourdes kusumadiNo ratings yet
- Blood Pressure Cardiac Output X Peripheral ResistanceDocument52 pagesBlood Pressure Cardiac Output X Peripheral Resistancelourdes kusumadiNo ratings yet
- Lo Hemato Week 4 1. DDX BAK Berdarah - Apa Aja Yang DinilaiDocument4 pagesLo Hemato Week 4 1. DDX BAK Berdarah - Apa Aja Yang Dinilailourdes kusumadiNo ratings yet
- Task 3Document12 pagesTask 3lourdes kusumadiNo ratings yet
- Untitled PDFDocument15 pagesUntitled PDFlourdes kusumadiNo ratings yet
- ST Francis Methodist School Atar Biology Task 2 Genetic Engineering - Creation of Black RosesDocument9 pagesST Francis Methodist School Atar Biology Task 2 Genetic Engineering - Creation of Black Roseslourdes kusumadiNo ratings yet
- Graph For Bio Task 1Document2 pagesGraph For Bio Task 1lourdes kusumadiNo ratings yet
- BME Task 1Document10 pagesBME Task 1lourdes kusumadiNo ratings yet
- How Is Woodside Maximizing Their Business?Document2 pagesHow Is Woodside Maximizing Their Business?lourdes kusumadiNo ratings yet
- Critical Thinking Assignment Name: Lourdes Joanna Kusumadi NIM: 01071180126 Batch: 2018Document2 pagesCritical Thinking Assignment Name: Lourdes Joanna Kusumadi NIM: 01071180126 Batch: 2018lourdes kusumadiNo ratings yet
- Anzac Day (Pg. 239) I. AuthorDocument5 pagesAnzac Day (Pg. 239) I. Authorlourdes kusumadiNo ratings yet
- Bookshelf - NBK132831, Bahan UL PDFDocument368 pagesBookshelf - NBK132831, Bahan UL PDFagung wiwinNo ratings yet
- Neuromyelitis OpticaDocument1 pageNeuromyelitis OpticaArun PonnaNo ratings yet
- Calciphylaxis - A Successful Outcome in Wound ManagementDocument1 pageCalciphylaxis - A Successful Outcome in Wound ManagementRobbyNo ratings yet
- PH CM 1 Cu 2 - Pharmacodynamics - 1Document10 pagesPH CM 1 Cu 2 - Pharmacodynamics - 1Chesca DomingoNo ratings yet
- NCP For CAP TB.Document5 pagesNCP For CAP TB.Cherry Ann BalagotNo ratings yet
- Adult Cardiac Arrest Algorithm: VF/PVT Asystole/PEADocument1 pageAdult Cardiac Arrest Algorithm: VF/PVT Asystole/PEAAlexis HospitalNo ratings yet
- TesticularDocument79 pagesTesticularAndryanto リクア SutantoNo ratings yet
- Immediate Nursing Care of The NewbornDocument29 pagesImmediate Nursing Care of The NewbornDrei Lanuzo100% (1)
- Figure 1. New Criteria For AKI Diagnosis Are Displayed. in Order To Diagnose AKIDocument8 pagesFigure 1. New Criteria For AKI Diagnosis Are Displayed. in Order To Diagnose AKIMayra Alejandra Prada SerranoNo ratings yet
- Syllabus of Paramedical Courses SINGHANIADocument355 pagesSyllabus of Paramedical Courses SINGHANIANitin GargNo ratings yet
- Stem Cell BookDocument20 pagesStem Cell Bookbabasolai83No ratings yet
- Lansoprazole Fast Disintegrating Tablet: A New Formulation For An Established Proton Pump InhibitorDocument5 pagesLansoprazole Fast Disintegrating Tablet: A New Formulation For An Established Proton Pump Inhibitorroy bangarNo ratings yet
- Prakriya Hospitals Investor Brochure - 2019Document19 pagesPrakriya Hospitals Investor Brochure - 2019Abhishek S AatreyaNo ratings yet
- Joint Effort For Elimination of Tuberculosis (Jeet)Document2 pagesJoint Effort For Elimination of Tuberculosis (Jeet)Arindam MoitraNo ratings yet
- Mims Abbreviation IndexDocument1 pageMims Abbreviation IndexHendry RamadhanNo ratings yet
- Oral Hygiene ProductsDocument8 pagesOral Hygiene ProductsMr.ShazNo ratings yet
- VaccinationsDocument141 pagesVaccinationsdrmalsharrakhi_32794No ratings yet
- Referat GBSDocument12 pagesReferat GBSSoraya Dwi KhairunnisaNo ratings yet
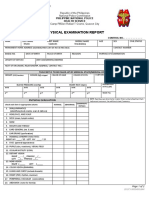
- Physical Examination Report: Philippine National Police Health ServiceDocument2 pagesPhysical Examination Report: Philippine National Police Health Servicelara michelleNo ratings yet
- A 2 6 Nle PointersDocument29 pagesA 2 6 Nle PointersAira Shane MargesNo ratings yet
- Bachelor of Science in Nursing: Care of Mother and Child and AdolescentDocument12 pagesBachelor of Science in Nursing: Care of Mother and Child and AdolescentJaja ManezNo ratings yet
- Planning An Imaging Department - Express HealthcareDocument8 pagesPlanning An Imaging Department - Express HealthcareSatish ReddyNo ratings yet
- Overseas Student Health Cover WADocument3 pagesOverseas Student Health Cover WAweb supportNo ratings yet
- 2003 - A Validation Study of The Hospital Anxiety and Depression Scale (HADS) in A Spanish Population PDFDocument7 pages2003 - A Validation Study of The Hospital Anxiety and Depression Scale (HADS) in A Spanish Population PDFVíctor MJNo ratings yet
- LECTURE ON Acid-Base BalanceDocument229 pagesLECTURE ON Acid-Base BalanceNayyer Khan100% (1)
- Biology Investigatory Project Class XII 2.ODocument25 pagesBiology Investigatory Project Class XII 2.OYash WardhanNo ratings yet
- EDUC9 Module 13Document5 pagesEDUC9 Module 13Jomarc Cedrick Gonzales100% (1)
- Rickets: Dr. Yasna Kibria MD Resident (Phase A) Department of Radiology and Imaging BsmmuDocument43 pagesRickets: Dr. Yasna Kibria MD Resident (Phase A) Department of Radiology and Imaging BsmmuYasna KibriaNo ratings yet
- Cefazolin Sodium AncefDocument1 pageCefazolin Sodium AncefKristi WrayNo ratings yet