You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Module in Defferentiating Bias and PrejudiceDocument16 pagesModule in Defferentiating Bias and PrejudiceLudovina Calcaña95% (22)
- Kelompok 2 Stated Detail QuestionsDocument14 pagesKelompok 2 Stated Detail QuestionsVeronicaNo ratings yet
- Tuga2 Eliza Veronica 1708208201Document4 pagesTuga2 Eliza Veronica 1708208201VeronicaNo ratings yet
- Eliza Veronica Tugas 8Document1 pageEliza Veronica Tugas 8VeronicaNo ratings yet
- COVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesDocument10 pagesCOVID-19 Infection: Origin, Transmission, and Characteristics of Human CoronavirusesVeronicaNo ratings yet
- Hiv Live 2Document10 pagesHiv Live 2VeronicaNo ratings yet
- Corporation Code of The PhilippinesDocument36 pagesCorporation Code of The PhilippinesPaul Dean MarkNo ratings yet
- Operations Management: Operations Excellence of Ambuja Cement LTDDocument6 pagesOperations Management: Operations Excellence of Ambuja Cement LTDPratyus Kumar PandaNo ratings yet
- Jupiter Bioscience Limited Andhra Pradesh IndiaDocument10 pagesJupiter Bioscience Limited Andhra Pradesh IndiaJupiter Bioscience LimitedNo ratings yet
- Exam Centre Bill Proforma NiosDocument24 pagesExam Centre Bill Proforma NiosAnji KaringuNo ratings yet
- Corrosion Strategy in Oil Field System 2020Document12 pagesCorrosion Strategy in Oil Field System 2020tugceNo ratings yet
- Module 3 (The Interns)Document6 pagesModule 3 (The Interns)Jayrald Mendoza50% (2)
- Prospect SRSKerlaDocument23 pagesProspect SRSKerlaSonal ShahNo ratings yet
- Wipro Online Assessment Syllabus - Elite National Talent Hunt'22Document2 pagesWipro Online Assessment Syllabus - Elite National Talent Hunt'22Just HereNo ratings yet
- The Ring's The Thing: Top: The 2016 UIL 2A State Volleyball ChampionshipDocument1 pageThe Ring's The Thing: Top: The 2016 UIL 2A State Volleyball ChampionshipAna CosinoNo ratings yet
- PDF - English Grade 8 - Unit - 18 - West Asian Literature 3 TopicsDocument24 pagesPDF - English Grade 8 - Unit - 18 - West Asian Literature 3 TopicsArabella100% (2)
- 048 InternationalLaw Admiralty Maritime PDFDocument228 pages048 InternationalLaw Admiralty Maritime PDF:Lawiy-Zodok:Shamu:-El100% (2)
- Automatic Hand DrierDocument27 pagesAutomatic Hand DrierEmiola Sunny Day JoshuaNo ratings yet
- Mercede ResumeDocument1 pageMercede Resumeapi-160000915No ratings yet
- Tips For Pop ArrangingDocument6 pagesTips For Pop ArrangingPlosytre Grostuna100% (1)
- Hack Literature ReviewDocument6 pagesHack Literature Reviewfeiaozukg100% (1)
- AoS Skaven Warscroll Card Plague MonksDocument1 pageAoS Skaven Warscroll Card Plague MonksEsh BleakeNo ratings yet
- Network Database ModelDocument7 pagesNetwork Database ModelArfaqammarNo ratings yet
- Betty Neuman: The System ModelDocument32 pagesBetty Neuman: The System ModelVincent PolicarNo ratings yet
- 4.production FunctionsDocument29 pages4.production FunctionsKanika BakshiNo ratings yet
- Absolute and Universal Moral PrinciplesDocument5 pagesAbsolute and Universal Moral PrinciplesLewmas UyimisNo ratings yet
- Vaccination Schedule Commercial LayerDocument3 pagesVaccination Schedule Commercial LayerBINAY KUMAR YADAVNo ratings yet
- 9e 01 Chap Student WorkbookDocument16 pages9e 01 Chap Student Workbookmocho.knabbis481No ratings yet
- Artificial Intelligence and Financial Services: Index TermsDocument12 pagesArtificial Intelligence and Financial Services: Index TermsMoncef ChorfiNo ratings yet
- Sample TG For MILDocument13 pagesSample TG For MILRavubyNo ratings yet
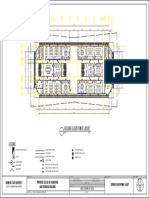
- E1 Ground Floor Power LayoutDocument1 pageE1 Ground Floor Power LayoutMark Anthony Mores FalogmeNo ratings yet
- Archetypes - Aboreal, Dragon, PlagueDocument5 pagesArchetypes - Aboreal, Dragon, PlagueTal Shimshon DekelNo ratings yet
- Justin Bankforts - Baltic Institute For Corporate GovernanceDocument29 pagesJustin Bankforts - Baltic Institute For Corporate GovernanceSabiedrība par atklātību - Delna / Transparency International LatviaNo ratings yet
- IMFA (Intermolecular Forces of Attraction) Surface TensionDocument27 pagesIMFA (Intermolecular Forces of Attraction) Surface TensionJoshua Gabriel Labaco100% (1)
- Mahesh Kumar GS - Technical Project Manager - Technical Lead - Senior Developer - DeveloperDocument9 pagesMahesh Kumar GS - Technical Project Manager - Technical Lead - Senior Developer - Developernagaraj.hNo ratings yet