You might also like
- Elements of ArgumentationDocument313 pagesElements of ArgumentationUdrescu Vasi91% (22)
- Kamigakari Expansion 1 - Requiem For The God SoulDocument177 pagesKamigakari Expansion 1 - Requiem For The God SoulLuciano Júnior100% (2)
- Sample CH 4 For Experimental ResearchDocument42 pagesSample CH 4 For Experimental ResearchDennis Esik MaligayaNo ratings yet
- Multigenre ProjectDocument13 pagesMultigenre Projectapi-429615976No ratings yet
- Car Sharing Report - Airbnb Business ModelDocument34 pagesCar Sharing Report - Airbnb Business Modelandra_36ukNo ratings yet
- Clinical Pilates Versus General Exercise For Chronic Low Back Pain: Randomized TrialDocument9 pagesClinical Pilates Versus General Exercise For Chronic Low Back Pain: Randomized TrialvistablancaNo ratings yet
- The Use of Pilates For Pain Control in Patients WiDocument9 pagesThe Use of Pilates For Pain Control in Patients WiOzgun OzturkNo ratings yet
- Clinical StudyDocument9 pagesClinical StudyJavierAntonioMéndezNo ratings yet
- Inspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled TrialDocument8 pagesInspiratory Muscle Training in Rehabilitation of Low Back Pain: A Randomized Controlled TrialMuhammad AbdullahNo ratings yet
- 2022 Article 14213Document16 pages2022 Article 14213Gabriel DelfinoNo ratings yet
- Rooks DDocument9 pagesRooks DDavid94No ratings yet
- Comparing The Pilates Method With No Exercise or Lumbar Stabilization For Pain and Functionality in Patients With Chronic Low Back Pain: Systematic Review and Meta-AnalysisDocument11 pagesComparing The Pilates Method With No Exercise or Lumbar Stabilization For Pain and Functionality in Patients With Chronic Low Back Pain: Systematic Review and Meta-AnalysisDinda BungaNo ratings yet
- Cairns 2006Document12 pagesCairns 2006David LorencNo ratings yet
- Pilates For Low Back Pain A Systematic RDocument5 pagesPilates For Low Back Pain A Systematic RNezrin BaxisliNo ratings yet
- Kinesiofobia y Catastrofismo Del Dolor y PilatesDocument7 pagesKinesiofobia y Catastrofismo Del Dolor y Pilatescecilia martinezNo ratings yet
- Artritis Idiopatica JuvenilDocument12 pagesArtritis Idiopatica JuvenilJhos_Leon15No ratings yet
- Exercise in Neuromuscular Disorders: A Promising InterventionDocument8 pagesExercise in Neuromuscular Disorders: A Promising InterventionTito AlhoNo ratings yet
- Rehabilitation and Fibromyalgia - Practice Essentials, Overview, Multidisciplinary RehabilitationDocument6 pagesRehabilitation and Fibromyalgia - Practice Essentials, Overview, Multidisciplinary RehabilitationAngie Paola RodriguezNo ratings yet
- Pilates 1Document12 pagesPilates 1aniakurowska2000No ratings yet
- JurnalDocument8 pagesJurnalAlifia RizqiNo ratings yet
- NEJM PrescribingTaiChiForFibromyalgiaDocument2 pagesNEJM PrescribingTaiChiForFibromyalgiaAdriano Carneiro da RochaNo ratings yet
- Lopes 2017Document7 pagesLopes 2017alonsoNo ratings yet
- A Randomized Controlled Trial of 8-Form Tai Chi Improves Symptoms and Functional Mobility in Fibromyalgia PatientsDocument10 pagesA Randomized Controlled Trial of 8-Form Tai Chi Improves Symptoms and Functional Mobility in Fibromyalgia Patientsnadia kurniaNo ratings yet
- PTJ 1275Document12 pagesPTJ 1275Taynah LopesNo ratings yet
- Journal of Bodywork & Movement TherapiesDocument11 pagesJournal of Bodywork & Movement TherapiesJorge GámezNo ratings yet
- PhysicalTreatments v4n1p25 en PDFDocument9 pagesPhysicalTreatments v4n1p25 en PDFFadma PutriNo ratings yet
- Geiger RDocument2 pagesGeiger Rprajaktab_14thseptbrNo ratings yet
- Medicine: The Effect of Lumbar Stabilization and Walking Exercises On Chronic Low Back PainDocument10 pagesMedicine: The Effect of Lumbar Stabilization and Walking Exercises On Chronic Low Back Painmatiinu matiinuNo ratings yet
- MSK Pain LBPDocument12 pagesMSK Pain LBPMd. Ariful IslamNo ratings yet
- P I M E, F, B, P: Ilates For Mprovement of Uscle Ndurance Lexibility Alance AND OstureDocument7 pagesP I M E, F, B, P: Ilates For Mprovement of Uscle Ndurance Lexibility Alance AND OstureDiana Magnavita MouraNo ratings yet
- PNF Ombro 04Document10 pagesPNF Ombro 04Isaias AlmeidaNo ratings yet
- Blankenhagen Lit ReviewDocument4 pagesBlankenhagen Lit Reviewapi-362395776No ratings yet
- Jurnal William Flexion Exercise PDFDocument13 pagesJurnal William Flexion Exercise PDFRennyRay67% (3)
- Core Training in Low Back Disorders Role of TheDocument6 pagesCore Training in Low Back Disorders Role of TheYoh ChenNo ratings yet
- Vikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundDocument8 pagesVikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundSekar AyuNo ratings yet
- Demi Rel 2019Document7 pagesDemi Rel 2019Luis Miguel Cardona VelezNo ratings yet
- Pregnancy Yoga TerjemahanDocument7 pagesPregnancy Yoga TerjemahanMelati Dwi PutriNo ratings yet
- Pilares Eficiente para El Suelo PelvicoDocument6 pagesPilares Eficiente para El Suelo PelvicoRitaNo ratings yet
- MJCU - Volume 89 - Issue September - Pages 1877-1882Document6 pagesMJCU - Volume 89 - Issue September - Pages 1877-1882Yusuf WildanNo ratings yet
- Pilates RandomizadoDocument13 pagesPilates RandomizadorodrigueuresNo ratings yet
- Ultrasound Evaluation of The Abdominal Wall and Lumbar Multifidus Muscles in Participants Who Practice Pilates: A 1-Year Follow-Up Case SeriesDocument11 pagesUltrasound Evaluation of The Abdominal Wall and Lumbar Multifidus Muscles in Participants Who Practice Pilates: A 1-Year Follow-Up Case SeriesDiana Magnavita MouraNo ratings yet
- Disability Predictors in Chronic Low Back Pain After Aquatic ExerciseDocument9 pagesDisability Predictors in Chronic Low Back Pain After Aquatic ExerciseDeby Tri LestariNo ratings yet
- George Et Al (2011) COREDocument12 pagesGeorge Et Al (2011) COREjoanNo ratings yet
- 2011-Khayambashi (1) 201201DD 023514Document8 pages2011-Khayambashi (1) 201201DD 023514Justine RamosNo ratings yet
- Physical Exercise As Therapy For Type 2 Diabetes MellitusDocument11 pagesPhysical Exercise As Therapy For Type 2 Diabetes MellitusOscar Castillo EspinozaNo ratings yet
- 2007 Lumbar Stabilization Part 2 PDFDocument9 pages2007 Lumbar Stabilization Part 2 PDFPatricia Andrea Acevedo ArancibiaNo ratings yet
- Scapular Muscle Rehabilitation Exercises in Overhead Athletes With Impingement SymptomsDocument10 pagesScapular Muscle Rehabilitation Exercises in Overhead Athletes With Impingement SymptomsTheologos PardalidisNo ratings yet
- BRS 0b013e3181b315ccDocument26 pagesBRS 0b013e3181b315ccharshadpardeshi45No ratings yet
- Low Back PainDocument9 pagesLow Back PaintamiNo ratings yet
- Graham - A Prospective Study of Physiotherapist Prescribed Community Based Exercise in Inflammatory Peripheral NeuropathyDocument8 pagesGraham - A Prospective Study of Physiotherapist Prescribed Community Based Exercise in Inflammatory Peripheral NeuropathykarinaNo ratings yet
- Effectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFDocument5 pagesEffectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFFelipe solis jimenez100% (1)
- Effects On Training and Detraining On Physical Function Control of Diabetes andDocument6 pagesEffects On Training and Detraining On Physical Function Control of Diabetes andMilenckaVidalConsiglieriNo ratings yet
- Pedlar Literature ReviewDocument7 pagesPedlar Literature Reviewapi-669451419No ratings yet
- Test Exercitii SpondiDocument9 pagesTest Exercitii Spondipanaghia.marian.17No ratings yet
- Bernard 2020Document11 pagesBernard 2020JesusNavarrete97No ratings yet
- Exercise and DepressionDocument5 pagesExercise and DepressionDumitrescu TinaNo ratings yet
- Pilates Exercises: Effects of Pilates Exercise Programs in People With Chronic Low Back Pain A Systematic ReviewDocument2 pagesPilates Exercises: Effects of Pilates Exercise Programs in People With Chronic Low Back Pain A Systematic ReviewRevathy RNo ratings yet
- Tomas Carus2007Document7 pagesTomas Carus2007Encarni Moreno CañasNo ratings yet
- Journal2 BADocument11 pagesJournal2 BAJam BerNo ratings yet
- Combination of Exercise and Advice Was Slightly Better Than Placebo For Subacute Low Back PainDocument1 pageCombination of Exercise and Advice Was Slightly Better Than Placebo For Subacute Low Back PainvinaymanNo ratings yet
- Efficacy of A Short-Term Physiotherapy Intervention Strategy in The Initial Stages of Multiple Sclerosis, A Case ReportDocument10 pagesEfficacy of A Short-Term Physiotherapy Intervention Strategy in The Initial Stages of Multiple Sclerosis, A Case ReportSailaja NandennagariNo ratings yet
- Sherin Seminar 2 Recent Adavances in Geriatric MSDsDocument44 pagesSherin Seminar 2 Recent Adavances in Geriatric MSDsANKITA SHETTYNo ratings yet
- "It's Important To Buy in To The New Lifestyle" Barriers and Facilitators of Exercise Adherence in A Population With Persistent Musculoskeletal PainDocument12 pages"It's Important To Buy in To The New Lifestyle" Barriers and Facilitators of Exercise Adherence in A Population With Persistent Musculoskeletal PainSteffani PinheiroNo ratings yet
- ShareefDocument12 pagesShareefParaschiva PîțuNo ratings yet
- The Art of PerfumeryDocument237 pagesThe Art of PerfumeryJavier Badawy100% (1)
- The Art of PerfumeryDocument237 pagesThe Art of PerfumeryJavier BadawyNo ratings yet
- The Study of Plant LifeDocument183 pagesThe Study of Plant LifeJavier BadawyNo ratings yet
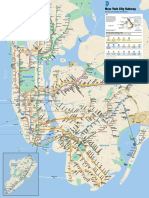
- New York Subway Map PDFDocument1 pageNew York Subway Map PDFSzabNo ratings yet
- 08 Nishimura IJSPP 2009 0139 497-508Document12 pages08 Nishimura IJSPP 2009 0139 497-508Javier BadawyNo ratings yet
- No Blueprint: Text by Robert Goethals, Photography by Robert HeineckenDocument7 pagesNo Blueprint: Text by Robert Goethals, Photography by Robert Heineckendaddypanama100% (1)
- State of Barangay Governance ReportDocument100 pagesState of Barangay Governance ReportBrgylusongNo ratings yet
- LogMate Configuration Changes For DeltaV 9 UpgradesDocument13 pagesLogMate Configuration Changes For DeltaV 9 UpgradesnegrinNo ratings yet
- BSC (Physics) SyllabusDocument16 pagesBSC (Physics) SyllabusAlok ThakkarNo ratings yet
- Introduction To Linear Regression and Correlation Analysis: ObjectivesDocument33 pagesIntroduction To Linear Regression and Correlation Analysis: ObjectivesJude Patrick SabaybayNo ratings yet
- MCQ DeepWater (2021 22)Document6 pagesMCQ DeepWater (2021 22)SAMBHAV PATNINo ratings yet
- Unicodebook PDFDocument73 pagesUnicodebook PDFaminerachedNo ratings yet
- 06a Practice Tests Set 3 - Paper 3HDocument22 pages06a Practice Tests Set 3 - Paper 3HafdsgafgNo ratings yet
- Corporate Design Manual: Big, Clever Digital MarketingDocument13 pagesCorporate Design Manual: Big, Clever Digital MarketingbigmouthmediaNo ratings yet
- Unit 1 Whole Numbers Objective QuestionsDocument4 pagesUnit 1 Whole Numbers Objective Questionskksangara100% (1)
- Black College Students in The Media OutlineDocument7 pagesBlack College Students in The Media OutlineParis ClarkNo ratings yet
- Pol6 - History of Pol. Thought Since 1890Document46 pagesPol6 - History of Pol. Thought Since 1890rabarber1900No ratings yet
- Green Bikes International Project Presentation FH WELS, AustriaDocument61 pagesGreen Bikes International Project Presentation FH WELS, AustriaManish AbrahamNo ratings yet
- Laski HauthorityDocument197 pagesLaski HauthorityerexwinNo ratings yet
- Easy CaptureDocument12 pagesEasy CaptureAndrea Sandoval RiquelmeNo ratings yet
- Usntps FTM 103Document684 pagesUsntps FTM 103unstamper100% (1)
- Project Specification: Saudi Arabian Oil CompanyDocument5 pagesProject Specification: Saudi Arabian Oil CompanyzhangNo ratings yet
- TKT Module 2 Selection and Use of Teaching Aids PDFDocument6 pagesTKT Module 2 Selection and Use of Teaching Aids PDFMona Gomez F.No ratings yet
- Enter Data: 2.109E+01 1.527E-04 2.937E-05 1.280E+01 3.969E-09Document3 pagesEnter Data: 2.109E+01 1.527E-04 2.937E-05 1.280E+01 3.969E-09Arcangelo Di TanoNo ratings yet
- T640 Integrated Loop ProcessorDocument5 pagesT640 Integrated Loop Processorరామకృష్ణ పాశలNo ratings yet
- Role ModelDocument61 pagesRole ModelGuru HegdeNo ratings yet
- III (2) Subjunctive Mood STDocument30 pagesIII (2) Subjunctive Mood STgocan12-1No ratings yet
- Types of Components and Objects To Be Measur EdDocument5 pagesTypes of Components and Objects To Be Measur EdRichard SugboNo ratings yet
- A Medical Error To Disclose or Not To Disclose 2155 9627-5-174Document3 pagesA Medical Error To Disclose or Not To Disclose 2155 9627-5-174Aduda Ruiz BenahNo ratings yet
- Unit 3 MKIS and Buyer BehaviorDocument38 pagesUnit 3 MKIS and Buyer BehaviorBHAKT Raj BhagatNo ratings yet