You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Borax ConspiracyDocument0 pagesThe Borax Conspiracyapi-240541707No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
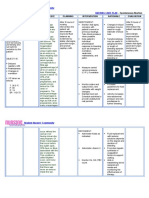
- Nursing Care Plan - Acute Pain Related To Surgical IncisionDocument2 pagesNursing Care Plan - Acute Pain Related To Surgical IncisionCamilogs80% (10)
- IPCRJan June2017Document4 pagesIPCRJan June2017Jenivic Empig Puedan50% (2)
- AETCOM Module IntroductionDocument30 pagesAETCOM Module Introductiondrmdsaeed78% (9)
- Pre Employment Medical Form PDFDocument1 pagePre Employment Medical Form PDFKristina Miller100% (1)
- Nursing Care Plan Output (NCP) 50 Points: Activity 14Document2 pagesNursing Care Plan Output (NCP) 50 Points: Activity 14Nathaniel Pulido50% (2)
- 1 s2.0 S2452247316600201 MainDocument3 pages1 s2.0 S2452247316600201 MainDiana BurbanoNo ratings yet
- 1 s2.0 S2452247316600201 MainDocument3 pages1 s2.0 S2452247316600201 MainDiana BurbanoNo ratings yet
- Art. OrlistatDocument6 pagesArt. OrlistatDiana BurbanoNo ratings yet
- Cleaning Validation in Pharmaceutical IndustriesDocument6 pagesCleaning Validation in Pharmaceutical IndustriesVimlesh Kumar PandeyNo ratings yet
- Activity and mRNA Levels of Enzymes Involved in Hepatic Fatty Acid Synthesis in Rats Fed NaringeninDocument7 pagesActivity and mRNA Levels of Enzymes Involved in Hepatic Fatty Acid Synthesis in Rats Fed NaringeninDiana BurbanoNo ratings yet
- Porfiri ADocument7 pagesPorfiri ADiana BurbanoNo ratings yet
- Articulo. Oxidacion de Alcoholes Con Peroxidos.Document2 pagesArticulo. Oxidacion de Alcoholes Con Peroxidos.Diana BurbanoNo ratings yet
- Annona SenegallensisDocument5 pagesAnnona SenegallensisDiana BurbanoNo ratings yet
- Larvicia ReticulataDocument5 pagesLarvicia ReticulataDiana BurbanoNo ratings yet
- Acti ReticulataDocument9 pagesActi ReticulataDiana BurbanoNo ratings yet
- Doing Work in A Certain Area .Especially in A Laboratory or in Any Work Place or Room ..Hazard and Risk Should Always Be ConsideredDocument36 pagesDoing Work in A Certain Area .Especially in A Laboratory or in Any Work Place or Room ..Hazard and Risk Should Always Be ConsideredJENA MAE FATAGANINo ratings yet
- Ahf Academy Lambrinou Case 1 17september2015.ppsxDocument36 pagesAhf Academy Lambrinou Case 1 17september2015.ppsxMWNo ratings yet
- TABLE 160-9: Treatment of DermatophytesDocument11 pagesTABLE 160-9: Treatment of DermatophytesIrsa SevenfoldismNo ratings yet
- Perioperative Nursing QuizDocument4 pagesPerioperative Nursing Quizgladz25100% (1)
- Track and Field Constitution 2021-2022 1Document7 pagesTrack and Field Constitution 2021-2022 1api-610935042No ratings yet
- Cataract PDFDocument8 pagesCataract PDFeashelNo ratings yet
- Gastroenteritis Case ReportDocument12 pagesGastroenteritis Case ReportjisooNo ratings yet
- Cook, J. D. (2003Document11 pagesCook, J. D. (2003Márcia LoureiroNo ratings yet
- Nursingcrib Com NURSING CARE PLAN Spontaneous AbortionDocument2 pagesNursingcrib Com NURSING CARE PLAN Spontaneous AbortionMina RacadioNo ratings yet
- Back To HydDocument2 pagesBack To Hydsai_ram2291175No ratings yet
- Meinhardt WaterborneDiseaseDocument3 pagesMeinhardt WaterborneDiseaseਮਕੁਮਾਰNo ratings yet
- PE UNIT 1 Active Recreation (Lifestyle and Weight Management)Document26 pagesPE UNIT 1 Active Recreation (Lifestyle and Weight Management)Charmaine RamosNo ratings yet
- Capillary Blood Glucose Performance Checklist: Numerical Rating Adjectival Description DescriptionDocument2 pagesCapillary Blood Glucose Performance Checklist: Numerical Rating Adjectival Description DescriptionAngeline NavarroNo ratings yet
- Test Metodu EN1276 PDFDocument13 pagesTest Metodu EN1276 PDFhcsoyleyiciNo ratings yet
- Moribund ICDSDocument114 pagesMoribund ICDSVikas SamvadNo ratings yet
- Pathophysiology DKADocument2 pagesPathophysiology DKALovely CacapitNo ratings yet
- COVID-19 Antigen Test Kit-Surge MedcialDocument16 pagesCOVID-19 Antigen Test Kit-Surge Medcialwalter sandoNo ratings yet
- FemTech Industry 2021 ReportDocument125 pagesFemTech Industry 2021 ReportMax 1549100% (1)
- MHPSSDocument11 pagesMHPSSVan TotNo ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
- Approved Harmonized National RD Agenda 2017-2022 PDFDocument90 pagesApproved Harmonized National RD Agenda 2017-2022 PDFJoemel Bautista100% (1)
- Inv PedDocument55 pagesInv PedrapayrapayNo ratings yet
- C0003 NHLDocument450 pagesC0003 NHLVasudev BhanajiNo ratings yet
- QuestionsDocument47 pagesQuestionsCharizza Yvette100% (1)