You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Oh Beaut Classic Lash Manual v9Document40 pagesOh Beaut Classic Lash Manual v9Jesica100% (4)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- National Geographic Reading Explorer 2nd Ed Book 5 - Unit 3Document62 pagesNational Geographic Reading Explorer 2nd Ed Book 5 - Unit 3Chantelle DUTOITSMITH100% (1)
- AMFEP-TEGEWA Industry Guidelines - Part I Textile Chemical FormulatorsDocument66 pagesAMFEP-TEGEWA Industry Guidelines - Part I Textile Chemical Formulatorsgurinder pal singhNo ratings yet
- AllergyDocument23 pagesAllergyAmbl GeronNo ratings yet
- Covid 19 Vaccine Orientation EditedDocument36 pagesCovid 19 Vaccine Orientation EditedLOVELY ANN RAMIREZNo ratings yet
- Chelsea SlechtaDocument1 pageChelsea Slechtaapi-458477176No ratings yet
- Different Approaches To Atopic Dermatitis by Allergists, Dermatologists, and PediatriciansDocument9 pagesDifferent Approaches To Atopic Dermatitis by Allergists, Dermatologists, and PediatriciansyelsiNo ratings yet
- Hanser Latex Examination ElbowDocument2 pagesHanser Latex Examination ElbowAndrian4979No ratings yet
- Practicaa 3 - BDocument4 pagesPracticaa 3 - BPaola Fiorella Quintana PérezNo ratings yet
- Tatalaksana Stomatitis Alergica Pada Penderita YanDocument7 pagesTatalaksana Stomatitis Alergica Pada Penderita YanAnshori 'arie' RohimiNo ratings yet
- Curs 4 - Alergia in EuropaDocument12 pagesCurs 4 - Alergia in EuropaBubulac AngelaNo ratings yet
- Trivedi, 2017 - Occupational Asthma - Diagnostic Challenges and Management DilemmasDocument7 pagesTrivedi, 2017 - Occupational Asthma - Diagnostic Challenges and Management DilemmasAditya IbrahimNo ratings yet
- Specification Sheet For Nitrile GlovesDocument4 pagesSpecification Sheet For Nitrile Glovesbagavan proNo ratings yet
- GROUP 10 Senstive Abt Food and Food AllergiesDocument16 pagesGROUP 10 Senstive Abt Food and Food AllergiesLilis nopita SarryNo ratings yet
- 2023 EAACI - Guidelines - Diagnosis - IgE-mediated - Food - AllergyDocument56 pages2023 EAACI - Guidelines - Diagnosis - IgE-mediated - Food - AllergyOlga CîrsteaNo ratings yet
- At The Doctor'sDocument2 pagesAt The Doctor'sІрина ГладійNo ratings yet
- The Role of Hydrolyzed Formula in Allergy Prevention by Michael D. CabanaDocument9 pagesThe Role of Hydrolyzed Formula in Allergy Prevention by Michael D. Cabanaali shahidNo ratings yet
- Antihistamine On ChildrenDocument10 pagesAntihistamine On ChildrenOpl OplNo ratings yet
- Radiology III ADocument4 pagesRadiology III AYousif AhmedNo ratings yet
- Nitrile Gloves Chemo Extended Cuff AloeTouchDocument4 pagesNitrile Gloves Chemo Extended Cuff AloeTouchSebastian CantilloNo ratings yet
- Irfanto, D. 2002. Algoritma Robotik. Jakarta: PT. Indo MediaDocument1 pageIrfanto, D. 2002. Algoritma Robotik. Jakarta: PT. Indo MediaAn Nisa AmeliaNo ratings yet
- Mikhaila Doyle - Observational Study Experimental DesignDocument3 pagesMikhaila Doyle - Observational Study Experimental Designapi-526180397No ratings yet
- Donning and Removing Sterile Gloves (Open Method) Preparation RationaleDocument2 pagesDonning and Removing Sterile Gloves (Open Method) Preparation RationalecharmainchavezNo ratings yet
- RLE 118 REVISED Case Scenario No. 10 Anaphylactic ShockDocument2 pagesRLE 118 REVISED Case Scenario No. 10 Anaphylactic ShockKiara Denise TamayoNo ratings yet
- Nursing Health HistoryDocument3 pagesNursing Health HistoryMea ParNo ratings yet
- Benefits of Growing GM CropsDocument2 pagesBenefits of Growing GM CropsPedrosa NardNo ratings yet
- Nursing Care Plan Profile: M.B (20 Yrs Old) Allergic RhinitisDocument1 pageNursing Care Plan Profile: M.B (20 Yrs Old) Allergic RhinitisMeccanazaren Susvilla Bojorque100% (1)
- The Epipen, A Case Study in Health System Dysfunction: by Aaron E. CarrollDocument3 pagesThe Epipen, A Case Study in Health System Dysfunction: by Aaron E. CarrollshubhamNo ratings yet
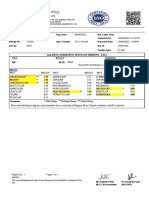
- Allergy Screening Tests (By Immuno - Eia)Document1 pageAllergy Screening Tests (By Immuno - Eia)Patel DhruviNo ratings yet
- Aanjan LabsDocument33 pagesAanjan LabsMeghanath PandhikondaNo ratings yet