You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- A Systematic Review of Guidelines For Managing Rheumatoid Arthritis Aneela Mian, Fowzia Ibrahim and David L. ScottDocument13 pagesA Systematic Review of Guidelines For Managing Rheumatoid Arthritis Aneela Mian, Fowzia Ibrahim and David L. ScottAdriana Estefanía HPNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Glucocorticoids in Management of Adult Rheumatoid Arthritiscurrentprescribing Practices and Perceptions of Physicians in India Glu 2329 8731 1000220Document6 pagesGlucocorticoids in Management of Adult Rheumatoid Arthritiscurrentprescribing Practices and Perceptions of Physicians in India Glu 2329 8731 1000220Rolando QuirozNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Glucocorticoids in Management of Adult Rheumatoid Arthritiscurrentprescribing Practices and Perceptions of Physicians in India Glu 2329 8731 1000220Document6 pagesGlucocorticoids in Management of Adult Rheumatoid Arthritiscurrentprescribing Practices and Perceptions of Physicians in India Glu 2329 8731 1000220Rolando QuirozNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Oxygen SupplementationDocument13 pagesOxygen SupplementationMr. LNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Oxygen SupplementationDocument13 pagesOxygen SupplementationMr. LNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Como Afecta ELWI Los LiquidosDocument12 pagesComo Afecta ELWI Los LiquidosBlanca Herrera MoralesNo ratings yet
- 10 Falsas Crrencuas en NefroDocument4 pages10 Falsas Crrencuas en NefroRolando QuirozNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- QX TLR9-Based Immunotherapy For TheDocument8 pagesQX TLR9-Based Immunotherapy For TheRolando QuirozNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Nfil 3Document23 pagesNfil 3Rolando QuirozNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- IshikawaDocument8 pagesIshikawaRolando QuirozNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Prevention & Early Outpatient Treatment Protocol For Covid-19Document2 pagesPrevention & Early Outpatient Treatment Protocol For Covid-19Arunima MajhiNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Welfare Checks and Therapeutic Risk Management.8Document5 pagesWelfare Checks and Therapeutic Risk Management.8Marco Dave Gutierrez ParedesNo ratings yet
- Radiation Therapist ResumeDocument8 pagesRadiation Therapist Resumeafjzdonobiowee100% (2)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Difference Between Generic and Brand NameDocument3 pagesDifference Between Generic and Brand NameNoor AliNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Introduction To PharmacologyDocument6 pagesIntroduction To PharmacologyJAMAL WARISNo ratings yet
- MainDocument10 pagesMainNataliaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
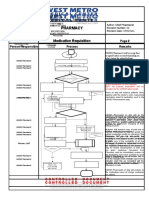
- Pharmacy Pharmacy: Medication Requisition Medication RequisitionDocument1 pagePharmacy Pharmacy: Medication Requisition Medication RequisitionSharie Grace ImlanNo ratings yet
- Approved Drug ProductsDocument1,298 pagesApproved Drug ProductsSaharNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Therapy For Narcissistic Personality DisorderDocument8 pagesTherapy For Narcissistic Personality DisorderhopeIshanzaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Energy and Information Medicine - MSchmiekeDocument13 pagesEnergy and Information Medicine - MSchmiekeMatsya das100% (2)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Kelcey ResumeDocument1 pageKelcey Resumeapi-419837296No ratings yet
- CND 4.medication & Dispensing ErrorDocument32 pagesCND 4.medication & Dispensing Errorlisnawati farmasicbthNo ratings yet
- Counter Transfer Vipin MishraDocument6 pagesCounter Transfer Vipin Mishravipin mishraNo ratings yet
- Chips Reference GuideDocument2 pagesChips Reference GuideMia JacksonNo ratings yet
- Ethical Issues PowerpointDocument12 pagesEthical Issues Powerpointapi-576929801No ratings yet
- Therapy ManualDocument52 pagesTherapy ManualcrisNo ratings yet
- Daftar Pustaka Sken 4Document4 pagesDaftar Pustaka Sken 4Allisya CarissaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Routes of Drug Administration and Evaluation PHC461Document15 pagesRoutes of Drug Administration and Evaluation PHC461beyonduckNo ratings yet
- Prashant Pps Front PgesDocument6 pagesPrashant Pps Front PgesM. Shoeb Sultan100% (1)
- Session 6Document4 pagesSession 6Dummy AccountNo ratings yet
- DownloadDocument1 pageDownloadAnderson Manuel Marquez NuñezNo ratings yet
- Navigating The Terrain of Oncology - A Comprehensive Guide To Understanding CancerDocument3 pagesNavigating The Terrain of Oncology - A Comprehensive Guide To Understanding CancerihealthmailboxNo ratings yet
- Clinical Pharmacology and Clinical PharmacyDocument8 pagesClinical Pharmacology and Clinical PharmacyRowena Concepcion Penafiel100% (1)
- Basic Principles of Compounding and DispensingDocument11 pagesBasic Principles of Compounding and DispensingAamna ShahNo ratings yet
- WHO Certificate E120 2019Document4 pagesWHO Certificate E120 2019Risen ChemicalsNo ratings yet
- Eacbt Sabbatino Mi 2010Document18 pagesEacbt Sabbatino Mi 2010Sonya SabbatinoNo ratings yet
- Hypnoanasthesia IndahDocument12 pagesHypnoanasthesia IndahRumah BidanNo ratings yet
- PSY224-The Theory and Practice of Group Psychotherapy, 6th Edition-Irvin Yalom, Molyn Leszcz-2020Document762 pagesPSY224-The Theory and Practice of Group Psychotherapy, 6th Edition-Irvin Yalom, Molyn Leszcz-2020Raamiah Edwards100% (1)
- Medical Issues: Acupuncture Might HelpDocument10 pagesMedical Issues: Acupuncture Might HelpMary B. SuazoNo ratings yet
- Miasms Syphilis Sycosis Maurice Fortier Bernoville.07345 - 2prefaceDocument3 pagesMiasms Syphilis Sycosis Maurice Fortier Bernoville.07345 - 2prefaceSantanu singhaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)