You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- His Personal AssistantDocument338 pagesHis Personal Assistantmanna_aiya100% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 10 FBS Q2M3 Tle10 - He - Food - Beverageservices - q2 - Mod3 - Takingfoodandbeverageorders - v3 (27 Pages)Document28 pages10 FBS Q2M3 Tle10 - He - Food - Beverageservices - q2 - Mod3 - Takingfoodandbeverageorders - v3 (27 Pages)LISANDRA JOMERO100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Eligibility CriteriaDocument13 pagesEligibility CriteriaArnab SahaNo ratings yet
- Highway Drainage - Lecture Version 073Document179 pagesHighway Drainage - Lecture Version 073Rajesh Khadka67% (3)
- Assignment On GST CouncilDocument4 pagesAssignment On GST CouncilSimran Kaur KhuranaNo ratings yet
- Pandora File RecoveryDocument3 pagesPandora File Recoveryzansue abutamNo ratings yet
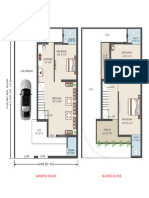
- 1102 SQ FTDocument1 page1102 SQ FTKanjariya YashvantNo ratings yet
- ECE 523: Synchronous Machine Steady-State Equivalent CircuitDocument8 pagesECE 523: Synchronous Machine Steady-State Equivalent CircuitJara FeyisaNo ratings yet
- Shadowlands Study GuideDocument8 pagesShadowlands Study GuideAnna ButnaruNo ratings yet
- Icao Worldwide Air Transport Conference (Atconf) Sixth MeetingDocument4 pagesIcao Worldwide Air Transport Conference (Atconf) Sixth MeetingAhmetBuğraÇetinNo ratings yet
- NitaiDocument622 pagesNitaiNitaiChand DasNo ratings yet
- (Aptitude) Percentage - Percentage To Fraction & Fraction To Percentage Conversion - RAVI MOHAN MISHRADocument1 page(Aptitude) Percentage - Percentage To Fraction & Fraction To Percentage Conversion - RAVI MOHAN MISHRAPeterGomesNo ratings yet
- ADV 02 - The Rise of Tiamat (8-15) Council Scorecard PDFDocument1 pageADV 02 - The Rise of Tiamat (8-15) Council Scorecard PDFGobitobiNo ratings yet
- Types of Storage DeviceDocument26 pagesTypes of Storage DeviceHarry ValeteNo ratings yet
- Maharaja Krishnakumarsinhji Bhavnagar University NIRF 2024 Ranking DataDocument8 pagesMaharaja Krishnakumarsinhji Bhavnagar University NIRF 2024 Ranking Dataashish goudarNo ratings yet
- In Service 2014Document20 pagesIn Service 2014Rao SgNo ratings yet
- La ST 18-22 P&i 88291003-548 06 PDFDocument1 pageLa ST 18-22 P&i 88291003-548 06 PDFAse MonNo ratings yet
- 4BE0 01 Rms BengaliDocument13 pages4BE0 01 Rms BengaliJohn HopkinsNo ratings yet
- Basic Circuit Design Revision - V2Document35 pagesBasic Circuit Design Revision - V2Rob PettitNo ratings yet
- Machine Learning Applications in Earthquake Engineering, A Literature ReviewDocument13 pagesMachine Learning Applications in Earthquake Engineering, A Literature ReviewEmby BinoeNo ratings yet
- General Specification: B. Plans and SpecificationsDocument5 pagesGeneral Specification: B. Plans and Specificationsmichael nabusNo ratings yet
- Conditionals (Download)Document6 pagesConditionals (Download)OmuletVerdeNo ratings yet
- Module Principles of Accounting Part II FinalDocument184 pagesModule Principles of Accounting Part II Finalyebegashet100% (15)
- Technicalproposal: For 750kva Substation EquipmentDocument4 pagesTechnicalproposal: For 750kva Substation EquipmentHarun MohamodNo ratings yet
- Picric Acid Method For Determining Weak Acid Dissociable WAD CyanideDocument3 pagesPicric Acid Method For Determining Weak Acid Dissociable WAD Cyanidemehdad xaliliNo ratings yet
- Ref.: SC/1017155/GGN/CRMIO/2019 Date: 08-Feb-2019: This Is A System Generated Letter and Does Not Require Any SignaturesDocument2 pagesRef.: SC/1017155/GGN/CRMIO/2019 Date: 08-Feb-2019: This Is A System Generated Letter and Does Not Require Any Signaturesgajala jamirNo ratings yet
- HIIT - Google SearchDocument1 pageHIIT - Google Searchpj villadolidNo ratings yet
- Belle MarianoDocument2 pagesBelle MarianoCorona VirusNo ratings yet
- Samsung BD h5900 BD h5500 BD Hm59 BD Hm59cDocument65 pagesSamsung BD h5900 BD h5500 BD Hm59 BD Hm59cMiguel Angel CarbonellNo ratings yet
- Call Deposit Receipt Meezan BankDocument22 pagesCall Deposit Receipt Meezan BankNabeel KhanNo ratings yet