You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- CCHU9021 Final Exam PaperDocument7 pagesCCHU9021 Final Exam PaperKaren TseNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Geriatric NeuropsychDocument480 pagesGeriatric NeuropsychSergio García100% (2)
- Job Search AssigmentDocument3 pagesJob Search Assigmentapi-607421876No ratings yet
- Drugs Acting On The Respiratory SystemDocument13 pagesDrugs Acting On The Respiratory SystemNathalie kate petallarNo ratings yet
- Trauma Evaluation and Management: Early Care of The Injured PatientDocument130 pagesTrauma Evaluation and Management: Early Care of The Injured PatienttesfahuntekleNo ratings yet
- Ear Drops Safety Data SheetDocument5 pagesEar Drops Safety Data SheetShehzadNo ratings yet
- Vihaan: Rehabilitation CentreDocument21 pagesVihaan: Rehabilitation Centreayush_agmNo ratings yet
- 4020 Assessment 4 Instructions - Improvement Plan Tool Kit - ..Document4 pages4020 Assessment 4 Instructions - Improvement Plan Tool Kit - ..Sabahat BashirNo ratings yet
- Introduction of Vaccine Into Immunization Programmes: Haemophilus Influenzae Type BDocument32 pagesIntroduction of Vaccine Into Immunization Programmes: Haemophilus Influenzae Type BAlphasera WiranandesNo ratings yet
- Psoriatic Arthritis Nature ReviewDocument17 pagesPsoriatic Arthritis Nature ReviewJose Shaid Delgado OlveraNo ratings yet
- EDSOP-8.4 Emergency Prep-Resp & Incident Management - SAMPLEDocument5 pagesEDSOP-8.4 Emergency Prep-Resp & Incident Management - SAMPLEafi pucca100% (1)
- Cardiac System AssessmentDocument14 pagesCardiac System AssessmentValarmathi100% (1)
- Benefits of Yoga PDFDocument2 pagesBenefits of Yoga PDFHarikrishna GopalakrishnanNo ratings yet
- Chromosomal Analysis of Mentally Retarded Children With MicrocephalyDocument12 pagesChromosomal Analysis of Mentally Retarded Children With MicrocephalyWiyosa RusdiNo ratings yet
- PsychiatryDocument7 pagesPsychiatryraluca.motorgaNo ratings yet
- Neurorehabilitation 1Document439 pagesNeurorehabilitation 1Duncan D'AmicoNo ratings yet
- Labcorp VoucherDocument2 pagesLabcorp Voucherjesse.777No ratings yet
- NAGPUR QUARANTINE LIST Police STN WiseDocument37 pagesNAGPUR QUARANTINE LIST Police STN Wiseabhijeet singh amarnathNo ratings yet
- Bernstein McNally 2018 Behaviour Research and TherapyDocument8 pagesBernstein McNally 2018 Behaviour Research and TherapyIordache LarisaNo ratings yet
- Capitalism's Care Problem: Some Traces, Fixes, and PatchesDocument28 pagesCapitalism's Care Problem: Some Traces, Fixes, and PatchesPatoEnCaralibroNo ratings yet
- Individuals With Disabilities Education Act2018Document9 pagesIndividuals With Disabilities Education Act2018vera marie pascualNo ratings yet
- RAMOS, LOUWELLA 2 BN International Health Information Regulatory BodiesDocument2 pagesRAMOS, LOUWELLA 2 BN International Health Information Regulatory BodiesLouwella RamosNo ratings yet
- Savina 300 BrochureDocument8 pagesSavina 300 BrochureRafa Tejeda100% (1)
- Workplace Safety EditedDocument19 pagesWorkplace Safety EditedRio Moseh ErikNo ratings yet
- Malingering 4Document7 pagesMalingering 4Vedora Angelia GultomNo ratings yet
- Malaysian Breastfeeding Peer Counselor Program Module (English) v2010-05Document110 pagesMalaysian Breastfeeding Peer Counselor Program Module (English) v2010-05Malaysian Breastfeeding Peer Counselor Program100% (1)
- Palliative Care in India: Santosh K. Chaturvedi Prabha S. ChandraDocument4 pagesPalliative Care in India: Santosh K. Chaturvedi Prabha S. ChandraJisha SreekumarNo ratings yet
- Paint WorkDocument1 pagePaint WorkNarender BhardwajNo ratings yet
- Policy - Partners or Support People Staying Overnight at Wellington HospitalDocument3 pagesPolicy - Partners or Support People Staying Overnight at Wellington HospitalStuff NewsroomNo ratings yet
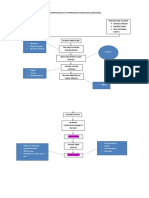
- Pathophysiology of Hypertensive Cardiovascular Disease: Chest Pain Muscle Weakness Shortness of BreathDocument2 pagesPathophysiology of Hypertensive Cardiovascular Disease: Chest Pain Muscle Weakness Shortness of BreathCyril Jane Caanyagan AcutNo ratings yet