You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- PSYC 2051 MidtermDocument7 pagesPSYC 2051 Midtermshreychadha5No ratings yet
- Handbook of Operant Behavior - TextDocument701 pagesHandbook of Operant Behavior - TextBeto RV100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Hernia PathophysiologyDocument1 pageHernia PathophysiologyIvan Louise Fajardo Maniquiz86% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Acute Respiratory DistressDocument2 pagesAcute Respiratory Distressminaanne100% (3)
- Chapter 1 Meat Inspection ProceduresDocument28 pagesChapter 1 Meat Inspection ProceduresJanice Li100% (3)
- Invasive Ductal CarcinomaDocument51 pagesInvasive Ductal CarcinomaGiselle Eclarino100% (2)
- Disorders of Acid Base BalanceDocument1 pageDisorders of Acid Base BalanceLyn Domingo EllaquezNo ratings yet
- Concept Map - Human Nervous SystemDocument1 pageConcept Map - Human Nervous SystemMENCHIE CORPUZNo ratings yet
- PHY3171 Lecture 1Document6 pagesPHY3171 Lecture 1PatrickNo ratings yet
- IAL Biology SB2 Assessment 8BDocument3 pagesIAL Biology SB2 Assessment 8BsalmaNo ratings yet
- 病理國考複習 PDFDocument61 pages病理國考複習 PDFAnonymous ZUQcbcNo ratings yet
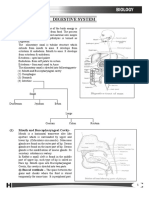
- Mammalian System-01 (Digestive System)Document35 pagesMammalian System-01 (Digestive System)Saumya99No ratings yet
- How To Apply Essential Oils For Chakra BalancingDocument2 pagesHow To Apply Essential Oils For Chakra BalancingAnumeha Jindal100% (1)
- 746259ku PDFDocument13 pages746259ku PDFTinkuNo ratings yet
- Pelvis and Perinium 2019Document59 pagesPelvis and Perinium 2019Vuluwa George100% (1)
- Module 12 Physical Development of Infants and Toddlerhood 1Document47 pagesModule 12 Physical Development of Infants and Toddlerhood 1Emely Manuel100% (8)
- Practical Guide To Plyometric IntensityDocument5 pagesPractical Guide To Plyometric IntensityEmiliano BezekNo ratings yet
- Anxiolytic-Antidepressant Activity of Glycowithanolides: An Experimental StudyDocument7 pagesAnxiolytic-Antidepressant Activity of Glycowithanolides: An Experimental StudynikuNo ratings yet
- Yoga For SeniorsDocument49 pagesYoga For SeniorsDr Srinivasan Nenmeli -KNo ratings yet
- Alternative Italian DictionaryDocument29 pagesAlternative Italian DictionaryAngelo PaganoNo ratings yet
- 27 ManeerattanarungrojDocument16 pages27 ManeerattanarungrojsanNo ratings yet
- Multiple ShoyshesDocument2 pagesMultiple ShoyshesJonathan Roy BombitaNo ratings yet
- Bandaging: Process of Covering A Wound and An Injured PartDocument23 pagesBandaging: Process of Covering A Wound and An Injured Partclarheena100% (1)
- Krimel SDocument2 pagesKrimel SBords ApaleNo ratings yet
- Anatomy and PhyDocument5 pagesAnatomy and PhydudzNo ratings yet
- Fertilization Fetal DevelopmentDocument97 pagesFertilization Fetal DevelopmentXo Yem100% (1)
- Burton Hunt Pony Club: Quiz 2021Document25 pagesBurton Hunt Pony Club: Quiz 2021api-306398192No ratings yet
- Proprioception ReflexesDocument20 pagesProprioception Reflexesthwiseman100% (1)
- Dhairya Mock Test-03Document7 pagesDhairya Mock Test-03Nirupam RoyNo ratings yet
- RetractileTestis PDFDocument1 pageRetractileTestis PDFYuda Saidillah RitongaNo ratings yet