You might also like
- Case Report: Hildhood Oral Lichen Planus A CaseDocument2 pagesCase Report: Hildhood Oral Lichen Planus A CaseFuad HasanNo ratings yet
- Median Rhomboid Glossitis With Palatal 'Kissing Lesion'-A Case ReportDocument4 pagesMedian Rhomboid Glossitis With Palatal 'Kissing Lesion'-A Case ReportAninda Wulan PradaniNo ratings yet
- Pediatric Oral Pigmented Lesions: A Short ReviewDocument5 pagesPediatric Oral Pigmented Lesions: A Short ReviewRoxana OneaNo ratings yet
- Irritational Fibroma A Case ReportDocument2 pagesIrritational Fibroma A Case ReportquikhaaNo ratings yet
- Oral Erythroplakia - A Case Report: Mahendra Patait, Urvashi Nikate, Kedar Saraf, Priyanka Singh and Vishal JadhavDocument4 pagesOral Erythroplakia - A Case Report: Mahendra Patait, Urvashi Nikate, Kedar Saraf, Priyanka Singh and Vishal JadhavhelmysiswantoNo ratings yet
- Endo - Perio Lesions A Diagnostic DilemmaDocument4 pagesEndo - Perio Lesions A Diagnostic DilemmaPinky TolaniNo ratings yet
- Pod PDFDocument3 pagesPod PDFTri Pamungkas IrawanNo ratings yet
- Dilemmatic Presentation of Linear Iga Disease: A Case ReportDocument4 pagesDilemmatic Presentation of Linear Iga Disease: A Case Reportharrystyles06969No ratings yet
- BCR 2013 200316Document4 pagesBCR 2013 200316ay lmaoNo ratings yet
- Odontogenic Myxoma A Rare Case ReportDocument3 pagesOdontogenic Myxoma A Rare Case Reportvictorubong404No ratings yet
- Rhomboid Glossitis: Synonyms Clinical FeaturesDocument3 pagesRhomboid Glossitis: Synonyms Clinical FeatureschakrawardanaNo ratings yet
- Jurnal 1Document4 pagesJurnal 1Abdul QaharNo ratings yet
- Odonto MaDocument5 pagesOdonto MaashariNo ratings yet
- Do Not Miss It"radix Entamolaris in Pediatric Patients An Endodontic Challenge: A Case Series and Review of Literature."Document5 pagesDo Not Miss It"radix Entamolaris in Pediatric Patients An Endodontic Challenge: A Case Series and Review of Literature."arshad khandayNo ratings yet
- Maxillofacial Radiographic Study of Gardner's Syndrome Presenting With Odontogenic Myxoma: A Rare Case ReportDocument6 pagesMaxillofacial Radiographic Study of Gardner's Syndrome Presenting With Odontogenic Myxoma: A Rare Case ReportAnne LydellNo ratings yet
- Article 1637738008Document5 pagesArticle 1637738008MutiaRamadhantiiNo ratings yet
- Jurnal Om AccDocument8 pagesJurnal Om Acckhairunnisa ANo ratings yet
- Case Report Torus Mandibula (IPM)Document2 pagesCase Report Torus Mandibula (IPM)fachira rusdiNo ratings yet
- Bilaterally Impacted Mandibular Supernumerary Premolars Associated With Unusual Clinical ComplicationsDocument5 pagesBilaterally Impacted Mandibular Supernumerary Premolars Associated With Unusual Clinical ComplicationsAira Grace PadillaNo ratings yet
- Al Ammar 2018Document9 pagesAl Ammar 2018Wayan Sutresna YasaNo ratings yet
- Median Rhomboid Glossitis in A Patient Undergoing Orthodontic TreatmentDocument4 pagesMedian Rhomboid Glossitis in A Patient Undergoing Orthodontic Treatmentandreia ichimNo ratings yet
- Sarcoidosis and Oral Manifestations For The DentistDocument32 pagesSarcoidosis and Oral Manifestations For The DentistJeff BurgessNo ratings yet
- Steroid Inhaler Therapy and Oral Manifestation Similar To Median Rhomboid GlossitisDocument3 pagesSteroid Inhaler Therapy and Oral Manifestation Similar To Median Rhomboid GlossitisRochmahAiNurNo ratings yet
- 1 s2.0 S0889540623002573 MainDocument12 pages1 s2.0 S0889540623002573 MainDANTE DELEGUERYNo ratings yet
- IndianJOralSci7151-2459446 064954Document3 pagesIndianJOralSci7151-2459446 064954Reza ChandraNo ratings yet
- Analisis Lesi Endo-Perio Di Periapikal Melalui Radiografi: Chrisna Ardhya Medika, Suhardjo Sitam, Lusi EpsilawatiDocument4 pagesAnalisis Lesi Endo-Perio Di Periapikal Melalui Radiografi: Chrisna Ardhya Medika, Suhardjo Sitam, Lusi EpsilawatiResa YudhistiNo ratings yet
- Investigations For Diseases of The Tongue A Review PDFDocument6 pagesInvestigations For Diseases of The Tongue A Review PDFShantanu DixitNo ratings yet
- Case Report: Idiopathic Gingival Fibromatosis Rehabilitation: A Case Report With Two-Year FollowupDocument6 pagesCase Report: Idiopathic Gingival Fibromatosis Rehabilitation: A Case Report With Two-Year FollowupauliaNo ratings yet
- Long Term Follow-Up of Oral Submucous Fibrosis Grade IV Case With A Versatile Nasolabial FlapA Case ReportDocument3 pagesLong Term Follow-Up of Oral Submucous Fibrosis Grade IV Case With A Versatile Nasolabial FlapA Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Benign Migratory Glossitis A Rare Presentation of A Common DisorderDocument3 pagesBenign Migratory Glossitis A Rare Presentation of A Common DisorderOjanNo ratings yet
- Coated TongueDocument4 pagesCoated TongueBulan MoonNo ratings yet
- Pi Is 0002934317306927Document2 pagesPi Is 0002934317306927DianNurlitaAnggrainiNo ratings yet
- Research Article: ISSN: 0975-833XDocument3 pagesResearch Article: ISSN: 0975-833XayuturaNo ratings yet
- Complex OdontomasDocument1 pageComplex OdontomasAnkita AroraNo ratings yet
- Case Presentation BSMMU As 3rd AuthorDocument4 pagesCase Presentation BSMMU As 3rd AuthorGovind ChaudharyNo ratings yet
- Variasi Normal Torus Mandibula OvilDocument2 pagesVariasi Normal Torus Mandibula OvilAqilahaisarNo ratings yet
- Reactive Lesions of Oral Cavity: A Retrospective Study of 659 CasesDocument6 pagesReactive Lesions of Oral Cavity: A Retrospective Study of 659 CasesGLORIA ISABEL VALDES CASTRONo ratings yet
- Oral Submucous Fibrosis With Angular Cheilitis - A Case Scenario With Present Concepts On Aetiology and ManagementDocument6 pagesOral Submucous Fibrosis With Angular Cheilitis - A Case Scenario With Present Concepts On Aetiology and ManagementInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 23 Case Rep1 Palatogingival GrooveDocument7 pages23 Case Rep1 Palatogingival GrooveDr.O.R.GANESAMURTHINo ratings yet
- Crid2022 5981020Document10 pagesCrid2022 5981020lily oktarizaNo ratings yet
- The International Journal of Periodontics & Restorative DentistryDocument10 pagesThe International Journal of Periodontics & Restorative DentistryLuis BeltranNo ratings yet
- Jurnal 1 PDFDocument4 pagesJurnal 1 PDFAnonymous Ro6cYoeNo ratings yet
- Oral Candidiasis - A Case ReportDocument4 pagesOral Candidiasis - A Case ReportDevinta RubaiNo ratings yet
- Periodontal Emergencies in General Practice: Primary Dental Journal June 2017Document7 pagesPeriodontal Emergencies in General Practice: Primary Dental Journal June 2017AmadeaNo ratings yet
- Crenated Tongue 2Document5 pagesCrenated Tongue 2Utami MayasariNo ratings yet
- Periodontal EmergenciesDocument7 pagesPeriodontal Emergenciesnandi prasetyaNo ratings yet
- Oral Mucosal Lesions in Children: Upine PublishersDocument3 pagesOral Mucosal Lesions in Children: Upine PublishersbanyubiruNo ratings yet
- 826-Abstract, Key Words, Introduction and Article Text and References-6236-1!10!20230324Document4 pages826-Abstract, Key Words, Introduction and Article Text and References-6236-1!10!20230324Ketut SariasihNo ratings yet
- Ijri - IJRI 286 19Document13 pagesIjri - IJRI 286 19krishnasantana1988No ratings yet
- Oral Health Status in Patients With Fixed OrthodonDocument5 pagesOral Health Status in Patients With Fixed OrthodonMitha Ari CahayaNo ratings yet
- Cavernous Hemangioma in The Floor of Oral Cavity Masquerading As A RanulaDocument5 pagesCavernous Hemangioma in The Floor of Oral Cavity Masquerading As A Ranula017Faradila Nayottama PutriNo ratings yet
- Lobular Capillary Hemangioma of TongueDocument3 pagesLobular Capillary Hemangioma of TongueShreya DasguptaNo ratings yet
- Conservative ManagementDocument4 pagesConservative ManagementFatima AliNo ratings yet
- Ejd - Ejd 261 16Document5 pagesEjd - Ejd 261 16Neggy YudibrataNo ratings yet
- Geographic Tongue: A Case Report With Review of LiteratureDocument3 pagesGeographic Tongue: A Case Report With Review of LiteratureDebby AyuNo ratings yet
- X RayDocument16 pagesX RaySaleha AlalwaniNo ratings yet
- The Dental Effects of Head and Neck Rhabdomyosarcoma Treatment - A Case SeriesDocument6 pagesThe Dental Effects of Head and Neck Rhabdomyosarcoma Treatment - A Case SeriesMohammad Abdulmon’emNo ratings yet
- Young2018 PDFDocument11 pagesYoung2018 PDFAndrew GarciaNo ratings yet
- Young Sjorgen's SDF GICDocument11 pagesYoung Sjorgen's SDF GICdr stoicaNo ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- 24 Bio Fertilization of BananaDocument6 pages24 Bio Fertilization of Bananamiceli57No ratings yet
- 12 Psychology - Meeting Life Challenges - Notes & Video LinkDocument11 pages12 Psychology - Meeting Life Challenges - Notes & Video LinkRamesh TalukdarNo ratings yet
- Annex I Summary of Product CharacteristicsDocument29 pagesAnnex I Summary of Product CharacteristicslisnerisNo ratings yet
- Canadian Pharmacy Review Ver1Document6 pagesCanadian Pharmacy Review Ver1Dr-Usman Khan30% (10)
- Calcium Hydroxide, Root ResorptionDocument9 pagesCalcium Hydroxide, Root ResorptionLize Barnardo100% (1)
- Test Bank For Microbiology Basic and Clinical Principles 1st Edition Lourdes P Norman MckayDocument36 pagesTest Bank For Microbiology Basic and Clinical Principles 1st Edition Lourdes P Norman Mckayshriekacericg31u3100% (43)
- Written Report Bio 150Document7 pagesWritten Report Bio 150hyebibieNo ratings yet
- Complications of DiabetesDocument3 pagesComplications of Diabetesa7wfNo ratings yet
- DR Ololade 038Document13 pagesDR Ololade 038Andrawus DanjumaNo ratings yet
- Guidelines EuromyastheniaDocument4 pagesGuidelines Euromyastheniadokter mudaNo ratings yet
- 2015 JC2 GP H1 Prelim PapersDocument357 pages2015 JC2 GP H1 Prelim PapersofficialJCUOLnotes100% (6)
- Lesson 5 Core Elements Evidenced Based Gerontological Nursing PracticeDocument38 pagesLesson 5 Core Elements Evidenced Based Gerontological Nursing PracticeSam GarciaNo ratings yet
- Paper Roleplay Group 3Document7 pagesPaper Roleplay Group 3Endah Ragil SaputriNo ratings yet
- 11 Retention of Maxillofacial Prosthesis Fayad PDFDocument7 pages11 Retention of Maxillofacial Prosthesis Fayad PDFMostafa Fayad50% (2)
- Farming Hirudo LeechesDocument46 pagesFarming Hirudo LeechesCatalin Cornel100% (1)
- Nur Writing - Marilyn JohnsonDocument4 pagesNur Writing - Marilyn Johnsonyinghua guo0% (1)
- Cytogenetics - Prelim TransesDocument15 pagesCytogenetics - Prelim TransesLOUISSE ANNE MONIQUE L. CAYLONo ratings yet
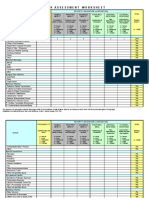
- IC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Document4 pagesIC Risk Assessment Worksheet - Kangas-V2.1-Aug.2010 1Juon Vairzya AnggraeniNo ratings yet
- Mood Disorders - Psychology ProjectDocument16 pagesMood Disorders - Psychology ProjectKanika Mathew100% (1)
- Nursing Management of HypertensionDocument152 pagesNursing Management of HypertensionEnfermeriaAncam100% (3)
- Physiology of The Cell: H. Khorrami PH.DDocument89 pagesPhysiology of The Cell: H. Khorrami PH.Dkhorrami4No ratings yet
- Cast and SplintsDocument58 pagesCast and SplintsSulabh Shrestha100% (2)
- Clinchers: RheumatologyDocument22 pagesClinchers: RheumatologyvarrakeshNo ratings yet
- DSM OcdDocument2 pagesDSM Ocdnmyza89No ratings yet
- Dula-Tungkulin o Gampanin NG ProduksyonDocument12 pagesDula-Tungkulin o Gampanin NG ProduksyonBernadette DuranNo ratings yet
- Adult Failure To ThriveDocument5 pagesAdult Failure To Thriveasmika danaNo ratings yet
- What Is Malnutrition?: WastingDocument6 pagesWhat Is Malnutrition?: WastingĐoan VõNo ratings yet
- Community Nutrition in Action An Entrepreneurial Approach 7th Edition Boyle Test BankDocument26 pagesCommunity Nutrition in Action An Entrepreneurial Approach 7th Edition Boyle Test BankJenniferWashingtonfbiqe100% (51)
- ACR-Global Hand Washing Day 2021Document2 pagesACR-Global Hand Washing Day 2021Katy Chenee Napao Perez100% (1)
- HEX PG SyllabusDocument124 pagesHEX PG SyllabusJegadeesan MuniandiNo ratings yet