Volume 6, Issue 9, September – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Oral Submucous Fibrosis with Angular Cheilitis –
A Case Scenario with Present Concepts on
Aetiology and Management
Dr. N. Santana M.D.S Dr. B. Elamparithi
Professor and Head 3rd Year Post Graduate
Department Of Oral Medicine and Radiology, Oral Medicine and Radiology
Ragas Dental College and Hospital, Chennai-119 Ragas Dental College and Hospital, Chennai-119
Dr. J. Sathish Kumar Dr. B. Pavana
3rd Year Post Graduate 3rd Year Post Graduate
Oral Medicine and Radiology Oral Medicine and Radiology
Ragas Dental College and Hospital, Chennai-119 Ragas Dental College and Hospital, Chennai-119
Abstract:- Oral submucous fibrosis (OSMF) is a Angular cheilitis (AC) or perleche is an inflammatory
increased risk of precancerous condition characterized reaction at the corners of the mouth that is clinically
by alterations in the connective tissue fibers of the characterized by cracks, erythematous inflammation with
lamina propria and deeper parts leading to stiffness of moist maceration, and ulceration on the commissures of the
the mucosa and restricted mouth opening. OSMF is a lip4.
chronic progressive disease that affects the oral mucosa
as well as the pharynx and the upper two-thirds of the Angular cheilitis is a wet environment for microbial
esophagus. The causative factors of OSMF are areca nut growth at the commissures of the lip licking ,such as
chewing, ingestion of chilies, genetic factors, habitual lip licking, thumb sucking or biting the corners of
immunologic processes, nutritional deficiencies, and the lip, and drooping of tissues at the angles of the mouth for
others. This study aims to discuss about the unique, case long periods of time has been play a role in development of
of OSMF with angular cheilitis. AC4
I. INTRODUCTION This condition is often associated with pain, irritation,
and occasionally bleeding, and it can impair mastication and
OSMF (Oral Submucosal Fibrosis) is a potentially speaking5. Both the oral submucous fibrosis and the angular
malignant disease that causes progressive epithelial fibrosis cheilitis in this case have a 5-year duration.
of oral soft tissues, mainly affects the population of Indian
subcontinent. It is a chronic, insidious, and incapacitating II. CASE REPORT
disease of the oral mucosa and oropharynx ,which
occasionally occurs in the larynx. OSMF, results in a A 55 year old male patient came to the department of
gradual deprivation of organizational activity, significant oral medicine with a chief complaint of missing tooth in his
stiffness, and, eventually, the inability to open the mouth1. upper front tooth region for the past 5 years. On general
examination pallor of conjunctiva with history of peptic
The World Health Organization's (WHO) definition of ulcer under medication for past 5 years, also have history of
oral precancerous lesions, "the systemic pathological burning sensation while consuming hot and spicy foods .On
condition of the oral mucosa associated with a significant intra oral examination of right buccal mucosa appears pale
increase in cancer risk," is very consistent with the features and blanched with inflamed hyperkeratotic patch was
of OSMF3. It is characterized by inflammation, increased present, which was extending from retromolar pad region to
submucosal collagen deposition, and the formation of commissure of lip, measuring about 4x1cm in size and also
fibrotic bands in the oral and para oral tissues2. white slough surrounded by erythematous zone in relation to
48 and examination of left buccal mucosa appears pale and
Continuous irreversible fibrosis of the submucosa blanched with inflamed hyperkeratotic patch was present
causes closed jaws, unable to eat the general spicy foods that ,which was extending from retromolar pad region to
people in the population who are accustomed to, and has commissure of lip, approximately size measuring about
increased risk of malicious transformation 3. Schwartz 4x2cm and also a white slough surrounded by erythematous
coined the term in 1952 after describing it as an oral fibrosis zone in relation to 38.
condition. "Atrophica idiopathica tropica muticae oris" is a
type of atrophica idiopathica tropica muticae oris2.
IJISRT21SEP599 www.ijisrt.com 977
Volume 6, Issue 9, September – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
On palpation of both right and left buccal mucosa Patient was under conservative management for 1
show the presence of fibrotic vertical bands extending from month and patient is prescribed with TAB.ZINCOVIT and
retromolar pad to commissure of lip region at the level of TAB.SMFIBRO once daily for 30 days and triamcinolone 1
occlusal plane, which is firm ,leathery in consistency and % and DOLO gel CT 10 gm for topical application. Pt
with no other secondary changes. reviewed after 4 months and Healing was satisfactory for
both oral submucous fibrosis and angular cheilitis , mouth
On examination of tongue mucosa show smooth opening was improved and also burning sensation was
,glossy erythematous ,de-papillated appearance in anterior reduced .
2/3rd and posterior 1/3rd region with hyperpigmentation and
blanching. All protrusive, retrusive, upward, right and left IV. DISCUSSION
lateral movements are normal. And palpation show the
presence of horizontal fibrotic bands present in lateral Oral submucous fibrosis was first reported in India as
border of tongue, which is firm, leathery in consistency. 2 cases in 1953 and also first coined the term by joshi 6 Oral
There is no tenderness on palpation with no secondary submucous fibrosis (OSF) is a high risk precancerous
changes present. condition characterized by changes in the connective tissue
fibers of the lamina propria and deeper parts leading to
Examination of lip mucosa reveal presence of stiffness of the mucosa and restricted mouth opening7.The
ulcerative fissures in right and left corner of the lip, there is most common initial symptoms of OSF are ulceration,
tenderness on palpation with no secondary changes present xerostomia, a burning sensation, and limited ability to open
.Upper and lower labial frenum, uvula, and floor of the the mouth. These symptoms interfere with the daily life
mouth also appears normal. basis to the patient and may leads to complications8&9
Based on the clinical features and according to WHO The pathogenesis of oral submucous fibrosis is not
classification (Passi D et al 2017) our case is classified as well elucidated, but it is believed to be a disease of
ORAL SUBMUCOUS FIBROSIS GRADE- ІІ23. multifactorial origin. Factors include areca nut chewing,
ingestion of chilies, genetic factors, immunologic processes,
III. DIFFERENTIAL DIAGNOSIS nutritional deficiencies, and others. These are observed
among patients that chewing of areca nut in the form of pan
Regarding the clinical findings of the disease such as masala or gutka for a long period of time and it causes
difficulty in mouth opening, the diagnosis that can be trauma to the oral mucosa, which leads to primary
thought of are localized scleroderma, OSMF and inflammatory reaction (mucositis).
erythroplakia. But after deliberating the history of having
habit of chronic alcoholism and looking at the clinical signs As numerous studies have shown, inflammatory
and symptoms, OSMF was confirmed as provisional cytokines are the initial process in oral submucous fibrosis,
diagnosis20. patient was advised for blood investigations and this is most likely the trigger mechanism in the early stages
also for biopsy. of the disease10. OSMF have a characteristic histological
appearance with complete lack of rete ridges and severely
Blood investigation show increased iron binding atrophied epithelium. There may be varying degrees of
capacity which indicates iron deficiency anemia and other epithelial atypia. The underlying lamina propria is severely
blood parameters are normal. Peripheral smear show hyalinized, with collagen homogeneity. It's possible that
hemoglobin level of 8.2mg/dl. Patient recalled after blood cellular elements and blood vessels will be diminished11. By
investigations for biopsy. Incisional biopsy was performed seeing the clinical feature angular Cheilitis we further
in the region of right buccal mucosa at the occlusal level diagnosed and confirmed that the patient has iron deficiency
under local anesthesia and sutures were placed. The biopsy anemia.
tissue was sent to the histopathological examination.
Angular cheilitis is an inflammatory disorder in which
The given soft tissue section shows an atrophic Para one or both angles of the mouth are erosively inflamed.
keratinized stratified squamous surface epithelium in Erythema, scaling, fissuring, and ulceration are common
association with a fibro vascular connective tissue exhibiting symptoms. Cheilitis can be caused by a number of things,
a dense diffuse mixed inflammatory cell infiltrate and mast including nutritional deficits, local and systemic causes, and
cells. The connective tissue also exhibits focal aggregation pharmacological adverse effects.12&13
of inflammatory cells and muscle fibers in the deeper part of
the tissue section. The focal areas of surface epithelium Nutritional deficiencies such as iron insufficiency and
exhibits basilar hyperplasia, hyperchromatism, cellular deficits of the B vitamins riboflavin (B2), niacin (B3),
vacuolation, basal cell degeneration and effacement of pyridoxine (B6), and cyanocobalamin (B12), account for
connective tissue interface. So we came to the 25% of all instances of angular cheilitis (B12)14.
histopathological diagnosis of epithelial dysplasia with mild Isotretinoin, sorafenib (antineoplastic kinase inhibitor), and
grading. Hence with final diagnosis of oral submucous ointments or creams like neomycin sulfate–polymyxin B
fibrosis with angular cheilitis. sulphate, bacitracin, idoxuridine, and steroids can all cause
angular cheilitis15.
IJISRT21SEP599 www.ijisrt.com 978
Volume 6, Issue 9, September – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
Lycopene is a type of antioxidant found mostly in iron balance in the average chronic gastrointestinal bleeding
tomatoes. It's an acyclic -carotene isomer. Its inhibitory patient24, they are considered first-line therapy.
effect on the abnormal proliferation of human abnormal
fibroblasts, as well as an elevation of lymphocyte stress Due to the grading of our case we suggest conservative
tolerance, have made it useful in OSMF. Because of its high treatment over the surgery.
amount of conjugated dienes, lycopene is one of the most
powerful antioxidants. It has a stronger ability to quench After persuading and counselling the patient to quit the
singlet oxygen than -carotene and -tocopherol.16 habit, a combination of medical therapy was recommended,
which included vitamin B complex capsules, antioxidants,
Epithelial atrophy results from juxta-epithelial and iron supplements, as well as oral physiotherapy, which
inflammation, increased fibrosis, and weakened vasculature, assisted in tissue remodeling to enhance mouth opening.20.
resulting in a burning sensation in the oral mucosa.
Lycopene aids epithelium regeneration by reducing the V. OUTCOME AND FOLLOW-UP
inflammatory and fibrotic processes17. Lycopene is safe and
has no side effects when consumed in a dietary dose18, and After a four-month follow-up, the patient's mouth
our research found that 8 mg/day in two divided doses is a opening had increased by 10 mm, owing to tissue
safe dose of lycopene with no side effects. As a result, remodeling achieved with a combination of medical therapy
lycopene is regarded as a successful, safe, and dependable and oral physiotherapy, which included vitamin B complex
drug in OSMF. capsules, antioxidants, and iron supplements. There was also
a reduction in the burning sensation when eating, and there
Short-acting (hydrocortisone), intermediate-acting were no clinical changes in the state of the diffuse
(triamcinolone), and long-acting (betamethasone and leukoplakic lesion on both the right and left buccal mucosa.
dexamethasone) glucocorticoids are used to treat OSMF. The patient was scheduled for three more follow-up visits at
Inhibition of inflammatory factor and increased apoptosis of three-month intervals, and he was told to stick to the same
inflammatory cells, resulting in partial relief of early stage treatment plan until he recovered20
OSMF symptoms. Also, twice weekly submucosal
injections of chymotrypsin (5000 IU), hyaluronidase (1500 VI. CONCLUSION
IU), and dexamethasone (4 mg) for 10 weeks. The current
notion is to employ mouth opening exercises followed by Asians have a betel nut chewing habit, which
intralesional injections into the fibrotic band every two contributes to OSMF. OSF disrupts collagen homeostasis,
weeks for 6 to 8 weeks25. increasing collagen production while decreasing collagen
clearance and causing structural and compositional
IFN is used to decrease fibroblast proliferation and abnormalities19
collagen synthesis while increasing collagenase production
and antifibrotic cytokines25. When intralesional IFN was The main problem in treating OSMF is that the patient
given to OSMF patients, it resulted in improved mouth is unaware of the areca nut and tobacco's side effects and
opening, mucosal suppleness, and a reduction in burning carcinogenic potential20. Many protocols for treating OSMF
sensation25. As an additional therapy for OSMF, symptoms have been proposed, and treatment regimens are
pentoxifylline 400mg was used three times daily for 7 still being developed21. Angular cheilitis, which typically
months. Pentoxifylline is a methylxanthine derivative with affects the lower lip with sparing of the corners of the
vasodilating characteristics, which promotes mucosal mouth, as well as dryness and cracking of the lips due to
vascularity. It suppresses leukocyte activity, changes nutritional deficiencies. Our patient's main clinical
fibroblast physiology, and stimulates fibronylysis25. manifestation of iron deficiency anemia was angular
cheilitis, emphasizing the importance of looking for iron
Ferrous iron supplements in the form of ferrous deficiency in patients who do not have a more obvious
fumarate, ferrous sulphate, and ferrous gluconate can be cause14 A 2 weeks follow up of Angular cheilitis patients
used to treat angular cheilitis24. Because oral iron with is recommended. This enables the health care provider
supplements are safe, inexpensive, and effective in restoring to analyze the success/effectiveness of the treatment given22.
IJISRT21SEP599 www.ijisrt.com 979
Volume 6, Issue 9, September – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
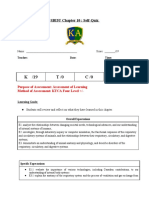
Pre Operative Pictures
Figure 1:- Presence of bands in the left buccal mucosa
Figure 2:- Presence of angular chielitis
IJISRT21SEP599 www.ijisrt.com 980
Volume 6, Issue 9, September – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
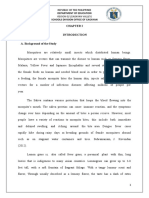
Biopsy Site
Figure 3:- Satisfactory healing in post operative pictures
A A
IJISRT21SEP599 www.ijisrt.com 981
Volume 6, Issue 9, September – 2021 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165
REFERENCES [15]. Yang CH, Lin WC, Chuang CK, et al. Hand-foot
skin reaction in patients treated with sorafenib: a
[1]. Chole RH, Patil R. Drug treatment of oral sub clinicopathological study of cutaneous
mucous fibrosis–a review. Int J Contemp Med Res. manifestations due to multitargeted kinase inhibitor
2016;3(4):996-8. therapy. Br J Dermatol 2008; 158(3):592–596
[2]. Oral submucous fibrosis: a contemporary narrative [16]. Arakeri, G., Patil, S., Maddur, N., Rao US, V.,
review with a proposed interprofessional approach Subash, A., Patil, S., … Brennan, P. A.
for an early diagnosis and clinical management (2020). Long‐term effectiveness of lycopene in the
Naman R. Rao1* , Alessandro Villa2,3, management of oral submucous fibrosis (OSMF): A
Chandramani B. More4 , Ruwan D. Jayasinghe5 , 3 year follow‐up study. Journal of Oral Pathology &
Alexander Ross Kerr6 and Newell W. Johnsonan MedicineSunderraj S, Sharma R, Agarwal V,
doi.org/10.1186/s40463-020-0399-7 Narang P, Reddy YG, Sharma AK. An i
[3]. Arakeri G, Brennan PA. Oral submucous fibrosis: an [17]. S, Sharma R, Agarwal V, Narang P, Reddy YG,
overview of the aetiology, pathogenesis, Sharma AK. An in-vivo study to determine the
classification, and principles of management. British efficacy of Lycopene as compared to multivitamin
Journal of Oral and Maxillofacial Surgery. 2013 Oct preparation on OMFS. J Indian Aca Oral Med
1;51(7):587-93. Radiol. 2012;24:190-193.
[4]. Angular Cheilitis - An Updated Overview of the [18]. Sanadi RM, Doshi M, Ambulgekar JR, Khambatta
Etiology, Diagnosis, and ManagementInternational X. Lycopene: it's role in health and disease. Int J
Journal of Dentistry and Oral Science (IJDOS) Pharm Sci Res. 2012;3(12):4578-4582.
ISSN: 2377-8075Anitha Krishnan Pandarathodiyil [19]. Yin-Hwa Shih 1,y, Tong-Hong Wang 2,3,4,5,y,
1* , Sukumaran Anil 2 , Srinivas Prasad Vijayan 3 Tzong-Ming Shieh 6,* and Yu-Hsin Tseng 7,*
[5]. Diet nutrition management for treatment of Review Oral Submucous Fibrosis: A Review of
angularcheilitis deseases in children I Gusti Ayu Ari Etiopathogenesis, Diagnosis, and Therapy.
Agung 1 , Dewa Made Wedagama 2 , G AA Hartini [20]. Oral submucous fibrosis: a premalignant condition
3 in a 14-year-old Indian girl Anshula Deshpande,
[6]. Haider SM, Merchant AT, Fikree FF, Rahbar MH. Shital Kiran, Steffi Dhillon, Rachappa Mallikarjuna
Clinical and func‐ tional staging of oral submucous doi:10.1136/bcr-2013-20078.
fibrosis. Br J Oral Maxillofac Surg. 2000;38(1):12‐ [21]. Current protocols in the management of oral
15. submucous fibrosis: An update Gururaj Arakeri1 |
[7]. Hazarey VK, Erlewad DM, Mundhe KA, Ughade Kirthi Kumar Rai2 | George Boraks3 | Shekar
SN.Oral submucous fibrosis: study of 1000 cases Gowda Patil4 | Abdulsalam S. Aljabab5 | M.A.W.
from central India. Journal of oral pathology & Merkx6 | Marco Carrozzo7 | Peter A. Brennan8.
medicine. 2007 Jan;36(1):127. [22]. Angular Cheilitis - An Updated Overview of the
[8]. Fang, C.Y.; Hsia, S.M.; Hsieh, P.L.; Liao, Y.W.; Etiology, Diagnosis, and Management Anitha
Peng, C.Y.; Wu, C.Z.; Lin, K.C.; Tsai, L.L.; Yu, Krishnan Pandarathodiyil1*, Sukumaran Anil2,
C.C. Slug mediates myofibroblastic differentiation Srinivas Prasad Vijayan3International Journal of
to promote fibrogenesis in buccal mucosa. J. Cell. Dentistry and Oral Science (IJDOS) ISSN: 2377-
Physiol. 2019, 234, 6721–6730 8075.
[9]. Angadi, P.V.; Rekha, K.P. Oral submucous fibrosis: [23]. Clinical Staging of Oral Submucous Fibrosis: A
A clinicopathologic review of 205 cases in Indians. ReviewShivakumar.G.C.,웋and Sahana.S.워
Oral Maxillofac. Surg. 2011, 15, 15–19
[10]. Ray JG, Chatterjee R, Chaudhuri K. Oral Departments of 웋Oral Medicine and Radiology,
submucous fibrosis: a global challenge. Rising and 워Public Health Dentistry, Peopleʼs Dental
incidence, risk factors, management, and research
priorities. Periodontology 2000. 2019 Academy, Peopleʼs Group, Bhanpur, Bhopal-
Jun;80(1):200-12. 462037 (M .P), India.
[11]. Kariya P, Khobragade V, Sura S, Singh S. No age [24]. Diagnosis and management of iron deficiency
predilection for a disease like OSMF. A case report anemia in the 21st century Terri D. Johnson-
of 5-year-old child. Journal of oral biology and Wimbley and David Y. Graham DOI: 10.1177/
craniofacial research. 2020 Apr 1;10(2):153-7. 1756283X11398736.
[12]. Park KK, Brodell RT, Helms SE. Angular cheilitis, [25]. Oral Submucous Fibrosis: Current Concepts on
part 2: nutritional, systemic, and drug-related causes Aetiology and Management – A Review Sadiya
and treatment. Cutis 2011; 88(1):27–32. Khan, Abhishek Sinha, Shiva Kumar1 , Haider Iqbal
pmid:21877503
[13]. Park KK, Brodell RT, Helms SE. Angular cheilitis,
part 1: local etiologies. Cutis 2011; 87(6):289–295.
pmid:21838086
[14]. Ayesh MH. Angular cheilitis induced by iron
deficiency anemia. Cleve Clin J Med. 2018 Aug
1;85(8):581-2.
IJISRT21SEP599 www.ijisrt.com 982
You might also like
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Oral Submucous FibrosisDocument5 pagesOral Submucous FibrosisHesti RNo ratings yet
- Long Term Follow-Up of Oral Submucous Fibrosis Grade IV Case With A Versatile Nasolabial FlapA Case ReportDocument3 pagesLong Term Follow-Up of Oral Submucous Fibrosis Grade IV Case With A Versatile Nasolabial FlapA Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oral Lesions in Leprosy Revisited: A Case Report: A. K. Dhawan, MD, Prashant Verma, MD, and S. Sharma, MDDocument2 pagesOral Lesions in Leprosy Revisited: A Case Report: A. K. Dhawan, MD, Prashant Verma, MD, and S. Sharma, MDOjanNo ratings yet
- Physiotherapy Improves Mouth Opening in OSMFDocument9 pagesPhysiotherapy Improves Mouth Opening in OSMFViral ParekhNo ratings yet
- Oral Pemphigus Vulgaris: Corresponding Author: K Subadra, Ksubadra@sriramachandra - Edu.inDocument12 pagesOral Pemphigus Vulgaris: Corresponding Author: K Subadra, Ksubadra@sriramachandra - Edu.inDiva AzariaNo ratings yet
- Ijss Mar Oa09Document10 pagesIjss Mar Oa09Subodh NanavatiNo ratings yet
- Phempigus Vulgaris PDFDocument6 pagesPhempigus Vulgaris PDFMochi Chim-ChimNo ratings yet
- Pedicle Tongue Flap Surgery Relieves Trismus in Oral Submucous FibrosisDocument4 pagesPedicle Tongue Flap Surgery Relieves Trismus in Oral Submucous FibrosisZuzu FinusNo ratings yet
- PV 1Document4 pagesPV 1Aing ScribdNo ratings yet
- Diagnostics of Oral Mucosae: Histology and Microbiology - Clinical RelevanceDocument14 pagesDiagnostics of Oral Mucosae: Histology and Microbiology - Clinical RelevanceGeorgi GugicevNo ratings yet
- Pak J Med Dent 2014 3 4 39 42Document6 pagesPak J Med Dent 2014 3 4 39 42DrSanaa AhmedNo ratings yet
- Medip,+692 2728 1 CEDocument2 pagesMedip,+692 2728 1 CElaluli lilulaNo ratings yet
- Case Report: Oral Lesions: The Clue To Diagnosis of Pemphigus VulgarisDocument4 pagesCase Report: Oral Lesions: The Clue To Diagnosis of Pemphigus Vulgarisgilang_8899No ratings yet
- Fulltext 2Document1 pageFulltext 2ashajangamNo ratings yet
- Clinical Staging of Oral Submucous Fibrosis: A Review: Shivakumar.G.C., and Sahana.SDocument4 pagesClinical Staging of Oral Submucous Fibrosis: A Review: Shivakumar.G.C., and Sahana.Smorza rahbrNo ratings yet
- Treatment of Mouth Breathing and Maxillary Anterior ProclinationDocument4 pagesTreatment of Mouth Breathing and Maxillary Anterior ProclinationVaniaNo ratings yet
- An Insight Into Pericoronitis PDFDocument4 pagesAn Insight Into Pericoronitis PDFNarissaporn ChaiprakitNo ratings yet
- Classification System For Oral Submucous Grading - A Review: B. PriyadharshniDocument5 pagesClassification System For Oral Submucous Grading - A Review: B. PriyadharshniAhsan KhanNo ratings yet
- Cuecumin On Osmf Systematic RevciewDocument1 pageCuecumin On Osmf Systematic RevciewAASHMINo ratings yet
- Palatal Perforation Case Report and Literature ReviewDocument4 pagesPalatal Perforation Case Report and Literature ReviewMaqbul AlamNo ratings yet
- Oral Sub Mucous Fibrosis PathoDocument2 pagesOral Sub Mucous Fibrosis PathoTsega SKNo ratings yet
- Ijdr 201723 01Document3 pagesIjdr 201723 01lily oktarizaNo ratings yet
- Cjim 4 793Document4 pagesCjim 4 793Mega WulandariNo ratings yet
- OsmdnDocument3 pagesOsmdnhaneefmdfNo ratings yet
- Rhadomyoma Mouth Floor OOOE 2010Document5 pagesRhadomyoma Mouth Floor OOOE 2010DrPrabhat Kumar TiwariNo ratings yet
- Referat 1Document3 pagesReferat 1Tupicica GabrielNo ratings yet
- Aggressive Periodontitis Guide for Dental StudentsDocument12 pagesAggressive Periodontitis Guide for Dental StudentsPatriciaXavier100% (1)
- Oral Submucous Fibrosis Stages and SymptomsDocument73 pagesOral Submucous Fibrosis Stages and SymptomsSarvari PaturiNo ratings yet
- Acharya 2011Document4 pagesAcharya 2011andreia ichimNo ratings yet
- Rare Case of Tongue ActinomycosisDocument3 pagesRare Case of Tongue ActinomycosisMazin Al KhateebNo ratings yet
- 2 ApikDocument5 pages2 ApikAhmad Syauqie Al MuhdarNo ratings yet
- Variasi Normal Rongga MulutDocument18 pagesVariasi Normal Rongga MulutRafi Kusuma Ramdhan SukonoNo ratings yet
- Oral PathologyDocument10 pagesOral PathologyManisha SardarNo ratings yet
- Stomatitis. Aetiology and A Review. Part 2. Oral Diseases Caused Candida SpeciesDocument7 pagesStomatitis. Aetiology and A Review. Part 2. Oral Diseases Caused Candida SpeciesIzzahalnabilah_26No ratings yet
- Osseous Choristoma of Tongue-Two Case Reports - Bhoj Raj Adhikari, Jun Sato, Yoshihiro Abiko Et AlDocument4 pagesOsseous Choristoma of Tongue-Two Case Reports - Bhoj Raj Adhikari, Jun Sato, Yoshihiro Abiko Et AlBhoj Raj AdhikariNo ratings yet
- Steroid Inhaler Therapy and Oral Manifestation Similar To Median Rhomboid GlossitisDocument3 pagesSteroid Inhaler Therapy and Oral Manifestation Similar To Median Rhomboid GlossitisRochmahAiNurNo ratings yet
- Pemfigus VulgarisDocument5 pagesPemfigus VulgarisAgus LarobuNo ratings yet
- Morsicatio Labiorum-LinguarumDocument3 pagesMorsicatio Labiorum-LinguarumPaola SilvaNo ratings yet
- Oral Submucous Fibrosis A Global Challenge Rising Incidence Risk Factors ManagementDocument13 pagesOral Submucous Fibrosis A Global Challenge Rising Incidence Risk Factors ManagementRAEDNo ratings yet
- Treatment of Lingual Traumatic Ulcer Accompanied With Fungal InfectionsDocument5 pagesTreatment of Lingual Traumatic Ulcer Accompanied With Fungal InfectionsYuganya SriNo ratings yet
- Pediatric Oral Pathology: Micro-Marsupialization for Mucus RetentionDocument4 pagesPediatric Oral Pathology: Micro-Marsupialization for Mucus RetentionmascoNo ratings yet
- 22-Submission File-35-1-10-20190811Document3 pages22-Submission File-35-1-10-20190811DhevNo ratings yet
- Oral Manifestations of Systemic Diseases A Review, 2014 PDFDocument9 pagesOral Manifestations of Systemic Diseases A Review, 2014 PDFDwi Indah LestariNo ratings yet
- Austin: An Unusual Manifestation of Cutaneous Sarcoidosis in The Oral CavityDocument2 pagesAustin: An Unusual Manifestation of Cutaneous Sarcoidosis in The Oral CavityRENITA USWATUN HASANAH 1No ratings yet
- 10 Common Superficial Tongue LesionsDocument9 pages10 Common Superficial Tongue LesionsAngga NNo ratings yet
- Fissured Tongue: A Case Report and Review of Literature: KeywordsDocument5 pagesFissured Tongue: A Case Report and Review of Literature: Keywordssiti baiq gadishaNo ratings yet
- Jcedv 10 I 5 P 495Document4 pagesJcedv 10 I 5 P 495Yohana SimanjuntakNo ratings yet
- Case Reports: Annals and Essences of DentistryDocument3 pagesCase Reports: Annals and Essences of DentistryxxxNo ratings yet
- Oral Submucous FibrosisDocument18 pagesOral Submucous FibrosisDrVaibhav ShrivastavaNo ratings yet
- "Camouflage Treatment in Adenoid Facies: Long Face Syndrome"-A Case Report. - Orthodontic Cyber JouDocument11 pages"Camouflage Treatment in Adenoid Facies: Long Face Syndrome"-A Case Report. - Orthodontic Cyber Joudrrajesh27100% (1)
- Jcad 13 6 48Document6 pagesJcad 13 6 48neetika guptaNo ratings yet
- Lingual Abscess-A Rarity: Sujata M. Byahatti, Mohammed S. H. IngafouDocument5 pagesLingual Abscess-A Rarity: Sujata M. Byahatti, Mohammed S. H. IngafouDinda rfNo ratings yet
- Pulpitis JurnalDocument2 pagesPulpitis JurnalIsmail YusufNo ratings yet
- Self - Limiting Cutaneous Pemphigus Preceding The Oral Lesions - A Case Report PDFDocument5 pagesSelf - Limiting Cutaneous Pemphigus Preceding The Oral Lesions - A Case Report PDFLing Pei ChengNo ratings yet
- Scientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportDocument6 pagesScientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportSasa AprilaNo ratings yet
- Oral Submucous Fibrosis As A Forerunner of Malignancy - A Case ReportDocument4 pagesOral Submucous Fibrosis As A Forerunner of Malignancy - A Case ReportAishwarya S. NairNo ratings yet
- Advancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisDocument8 pagesAdvancing Healthcare Predictions: Harnessing Machine Learning for Accurate Health Index PrognosisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Investigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatDocument16 pagesInvestigating Factors Influencing Employee Absenteeism: A Case Study of Secondary Schools in MuscatInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Exploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractDocument7 pagesExploring the Molecular Docking Interactions between the Polyherbal Formulation Ibadhychooranam and Human Aldose Reductase Enzyme as a Novel Approach for Investigating its Potential Efficacy in Management of CataractInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- An Analysis on Mental Health Issues among IndividualsDocument6 pagesAn Analysis on Mental Health Issues among IndividualsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolDocument31 pagesThe Relationship between Teacher Reflective Practice and Students Engagement in the Public Elementary SchoolInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIDocument6 pagesThe Making of Object Recognition Eyeglasses for the Visually Impaired using Image AIInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Terracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonDocument14 pagesTerracing as an Old-Style Scheme of Soil Water Preservation in Djingliya-Mandara Mountains- CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Dense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)Document2 pagesDense Wavelength Division Multiplexing (DWDM) in IT Networks: A Leap Beyond Synchronous Digital Hierarchy (SDH)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Harnessing Open Innovation for Translating Global Languages into Indian LanuagesDocument7 pagesHarnessing Open Innovation for Translating Global Languages into Indian LanuagesInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterDocument11 pagesThe Utilization of Date Palm (Phoenix dactylifera) Leaf Fiber as a Main Component in Making an Improvised Water FilterInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formulation and Evaluation of Poly Herbal Body ScrubDocument6 pagesFormulation and Evaluation of Poly Herbal Body ScrubInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diabetic Retinopathy Stage Detection Using CNN and Inception V3Document9 pagesDiabetic Retinopathy Stage Detection Using CNN and Inception V3International Journal of Innovative Science and Research TechnologyNo ratings yet
- Auto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETDocument6 pagesAuto Encoder Driven Hybrid Pipelines for Image Deblurring using NAFNETInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Impact of Digital Marketing Dimensions on Customer SatisfactionDocument6 pagesThe Impact of Digital Marketing Dimensions on Customer SatisfactionInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Electro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyDocument7 pagesElectro-Optics Properties of Intact Cocoa Beans based on Near Infrared TechnologyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Survey of the Plastic Waste used in Paving BlocksDocument4 pagesA Survey of the Plastic Waste used in Paving BlocksInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Automatic Power Factor ControllerDocument4 pagesAutomatic Power Factor ControllerInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Comparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightDocument4 pagesComparatively Design and Analyze Elevated Rectangular Water Reservoir with and without Bracing for Different Stagging HeightInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentDocument7 pagesCyberbullying: Legal and Ethical Implications, Challenges and Opportunities for Policy DevelopmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Explorning the Role of Machine Learning in Enhancing Cloud SecurityDocument5 pagesExplorning the Role of Machine Learning in Enhancing Cloud SecurityInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Design, Development and Evaluation of Methi-Shikakai Herbal ShampooDocument8 pagesDesign, Development and Evaluation of Methi-Shikakai Herbal ShampooInternational Journal of Innovative Science and Research Technology100% (3)
- Review of Biomechanics in Footwear Design and Development: An Exploration of Key Concepts and InnovationsDocument5 pagesReview of Biomechanics in Footwear Design and Development: An Exploration of Key Concepts and InnovationsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Navigating Digitalization: AHP Insights for SMEs' Strategic TransformationDocument11 pagesNavigating Digitalization: AHP Insights for SMEs' Strategic TransformationInternational Journal of Innovative Science and Research Technology100% (1)
- Studying the Situation and Proposing Some Basic Solutions to Improve Psychological Harmony Between Managerial Staff and Students of Medical Universities in Hanoi AreaDocument5 pagesStudying the Situation and Proposing Some Basic Solutions to Improve Psychological Harmony Between Managerial Staff and Students of Medical Universities in Hanoi AreaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Formation of New Technology in Automated Highway System in Peripheral HighwayDocument6 pagesFormation of New Technology in Automated Highway System in Peripheral HighwayInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- A Review: Pink Eye Outbreak in IndiaDocument3 pagesA Review: Pink Eye Outbreak in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Hepatic Portovenous Gas in a Young MaleDocument2 pagesHepatic Portovenous Gas in a Young MaleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Mobile Distractions among Adolescents: Impact on Learning in the Aftermath of COVID-19 in IndiaDocument2 pagesMobile Distractions among Adolescents: Impact on Learning in the Aftermath of COVID-19 in IndiaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Drug Dosage Control System Using Reinforcement LearningDocument8 pagesDrug Dosage Control System Using Reinforcement LearningInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- The Effect of Time Variables as Predictors of Senior Secondary School Students' Mathematical Performance Department of Mathematics Education Freetown PolytechnicDocument7 pagesThe Effect of Time Variables as Predictors of Senior Secondary School Students' Mathematical Performance Department of Mathematics Education Freetown PolytechnicInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Jaundice management strategiesDocument40 pagesJaundice management strategiesAdebisiNo ratings yet
- FERENAL, CLS Dummy ChartDocument4 pagesFERENAL, CLS Dummy ChartChristine Lorraine FerenalNo ratings yet
- DT 2N EU EN safetyDataSheet Sds 8799831064580 0 1Document12 pagesDT 2N EU EN safetyDataSheet Sds 8799831064580 0 1Jonatan BernalNo ratings yet
- Pedh ExamDocument12 pagesPedh ExamJames100% (2)
- Final AnnouncementDocument14 pagesFinal AnnouncementAziz AndriyantoNo ratings yet
- Croup: Assessment and ManagementDocument3 pagesCroup: Assessment and Managementsandra magdalenaNo ratings yet
- ABIS HSE L4 F 01 Risk Assessment FormDocument61 pagesABIS HSE L4 F 01 Risk Assessment FormOvais FarooqNo ratings yet
- Cardiothoracic SurgeryDocument24 pagesCardiothoracic SurgeryMARTINNo ratings yet
- Poisons of Plant OriginDocument46 pagesPoisons of Plant OriginThe AbyssinicansNo ratings yet
- Session 6 - Performing Abdominal ExaminationDocument33 pagesSession 6 - Performing Abdominal ExaminationOtsward OwdenNo ratings yet
- Leg Length Discrepancy (LLD) : H Fcmaf PM Ambcare AMB P AGE OFDocument1 pageLeg Length Discrepancy (LLD) : H Fcmaf PM Ambcare AMB P AGE OFanuragNo ratings yet
- Brain - Drain The Impact of Air Pulution On Firm PerformanceDocument69 pagesBrain - Drain The Impact of Air Pulution On Firm PerformancesinhNo ratings yet
- SBI3U Chapter 10 Self-Quiz ReviewDocument6 pagesSBI3U Chapter 10 Self-Quiz ReviewJannette JaneNo ratings yet
- A. Background of The Study: Department of Education Schools Division Office of CagayanDocument11 pagesA. Background of The Study: Department of Education Schools Division Office of CagayanJanjan GarciaNo ratings yet
- SBTP Annual Report 2018Document111 pagesSBTP Annual Report 2018RMCNo ratings yet
- Professional English For Physical SciencesDocument134 pagesProfessional English For Physical SciencesRavindranathan ArumugamNo ratings yet
- Prostate CancerDocument5 pagesProstate CancerBrilliant Osai-OyeteNo ratings yet
- User Manual: (High Intensity Focused Ultrasound)Document11 pagesUser Manual: (High Intensity Focused Ultrasound)Agha SoroushNo ratings yet
- BODYPUMP 100 Education Only - Print ReadyDocument5 pagesBODYPUMP 100 Education Only - Print ReadyNikolas MandilarasNo ratings yet
- Concise Guide Inbound ENGDocument1 pageConcise Guide Inbound ENGcsl K360No ratings yet
- Graham - A Prospective Study of Physiotherapist Prescribed Community Based Exercise in Inflammatory Peripheral NeuropathyDocument8 pagesGraham - A Prospective Study of Physiotherapist Prescribed Community Based Exercise in Inflammatory Peripheral NeuropathykarinaNo ratings yet
- Professional-grade dermatoscope for early skin cancer detectionDocument2 pagesProfessional-grade dermatoscope for early skin cancer detectionHemkerovner Keresztszegh von Kolowrat-KrakowskyNo ratings yet
- DOHaD and Birth Cohort ResearchDocument3 pagesDOHaD and Birth Cohort ResearchNguyễn Tiến HồngNo ratings yet
- 2017 Infectious Diseases Society of America's Clinical Practice Guidelines For Healthcare-Associated Ventriculitis and MeningitisDocument32 pages2017 Infectious Diseases Society of America's Clinical Practice Guidelines For Healthcare-Associated Ventriculitis and MeningitisEugen TarnovschiNo ratings yet
- Health7 Q4 Mod4 ProgramsAndPoliciesToPreventNon-communicableDiseases 05102021Document22 pagesHealth7 Q4 Mod4 ProgramsAndPoliciesToPreventNon-communicableDiseases 05102021kiahjessieNo ratings yet
- LECTURE - 8 Biomaterial PDFDocument34 pagesLECTURE - 8 Biomaterial PDFYoza FendrianiNo ratings yet
- Internal DiseaseDocument55 pagesInternal Diseaseshilpa sekhar278No ratings yet
- Mock test with 100 questions on pharmacy, medicine and IslamDocument34 pagesMock test with 100 questions on pharmacy, medicine and IslamSarahNo ratings yet
- Lec 10 AntiviralsDocument26 pagesLec 10 AntiviralsAiqa QaziNo ratings yet
- New Nursing Diagnoses 2012-2014Document11 pagesNew Nursing Diagnoses 2012-2014CarmenNoemiSantos100% (1)