You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sepsis Update 2018Document32 pagesSepsis Update 2018putri endah100% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Senarai Ho Banjir Medical 2014 PDFDocument4 pagesSenarai Ho Banjir Medical 2014 PDFAqua ForceNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Preterm Labor DahliaDocument4 pagesPreterm Labor DahliaAqua ForceNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Rapid Sequence Intubation: BY Budak KecikDocument25 pagesRapid Sequence Intubation: BY Budak KecikAqua ForceNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Rapid Sequence Intubation: BY Budak KecikDocument25 pagesRapid Sequence Intubation: BY Budak KecikAqua ForceNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Lactic Acidosis Update For Critical Care CliniciansDocument5 pagesLactic Acidosis Update For Critical Care CliniciansjohjossNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 10 1001@jama 2016 0287Document10 pages10 1001@jama 2016 0287ompardor7554No ratings yet
- ContohDocument4 pagesContohAqua ForceNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Att Letters SecDocument6 pagesAtt Letters SecAqua ForceNo ratings yet
- CampioneDocument1,652 pagesCampioneAqua ForceNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- UK National Guideline For The Management of Pelvic Inflammatory Disease 2011 PDFDocument18 pagesUK National Guideline For The Management of Pelvic Inflammatory Disease 2011 PDFPrissilmaTaniaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Coordinator of Six Year Prof Dr/Ahmed TarekDocument1 pageCoordinator of Six Year Prof Dr/Ahmed TarekAqua ForceNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Absenteeism Letter On Letterhead PDFDocument2 pagesAbsenteeism Letter On Letterhead PDFAqua ForceNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- List of Coordinators and Departments at HospitalDocument1 pageList of Coordinators and Departments at HospitalAqua ForceNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- VDFHGFHF Rtretr GR Df33254Document1 pageVDFHGFHF Rtretr GR Df33254Aqua ForceNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- NRDSDocument4 pagesNRDSAqua ForceNo ratings yet
- Approach To Chest PainDocument17 pagesApproach To Chest PainAqua ForceNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Emergency HTNDocument6 pagesEmergency HTNAqua ForceNo ratings yet
- Examples of OSCEDocument2 pagesExamples of OSCEAqua ForceNo ratings yet
- ReadmeDocument7 pagesReadmeLambourghiniNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
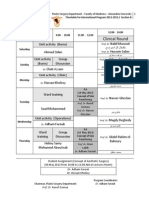
- Timetable For International Program 2012-2013 - Section BDocument1 pageTimetable For International Program 2012-2013 - Section BAqua ForceNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Torrent Downloaded FromDocument1 pageTorrent Downloaded FromAqua ForceNo ratings yet
- Cervicitis and VaginitisDocument18 pagesCervicitis and VaginitisAqua ForceNo ratings yet
- Examples of OSCEDocument2 pagesExamples of OSCEAqua ForceNo ratings yet
- Management of Head InjuriesDocument8 pagesManagement of Head InjuriesAqua ForceNo ratings yet
- Surgery TopicsDocument1 pageSurgery TopicsAqua ForceNo ratings yet
- Ent Past Years Question According To TopicsDocument32 pagesEnt Past Years Question According To Topicsmohamed100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- 243ear TraumaDocument33 pages243ear TraumaAqua ForceNo ratings yet
- Autoimmune Bullous DermatosesDocument143 pagesAutoimmune Bullous DermatosesAqua ForceNo ratings yet
- Angle Beam Transducer Dual ElementDocument5 pagesAngle Beam Transducer Dual ElementWilliam Cubillos PulidoNo ratings yet
- Structural Analysis of Mn(phen)3(CF3SO3)2 ComplexDocument7 pagesStructural Analysis of Mn(phen)3(CF3SO3)2 ComplexAnonymous 8pSaum8qNo ratings yet
- Miscellanea: Arab-Sasanian Copper P Esents Varie Ypo OgyDocument24 pagesMiscellanea: Arab-Sasanian Copper P Esents Varie Ypo Ogy12chainsNo ratings yet
- Unit 1 Lesson 2 PDFDocument20 pagesUnit 1 Lesson 2 PDFKristyll ArguellesNo ratings yet
- 3.0MP 4G Smart All Time Color Bullet Cam 8075Document2 pages3.0MP 4G Smart All Time Color Bullet Cam 8075IshakhaNo ratings yet
- Developmental AssessmentDocument15 pagesDevelopmental AssessmentShailesh MehtaNo ratings yet
- Centrifuge PDFDocument11 pagesCentrifuge PDFسراء حيدر كاظمNo ratings yet
- Montageanleitung sf25 35 enDocument20 pagesMontageanleitung sf25 35 enPaulo santosNo ratings yet
- Appointment Slip: 2 X 2 ID PictureDocument1 pageAppointment Slip: 2 X 2 ID PictureDarwin Competente LagranNo ratings yet
- SG CD FR 175 Levelness V 531 Lmi 001 Firmar SellarDocument1 pageSG CD FR 175 Levelness V 531 Lmi 001 Firmar SellarLuis VelazcogarciaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 19 G15 - Polycystic Ovary Syndrome v12.22.2021 1Document3 pages19 G15 - Polycystic Ovary Syndrome v12.22.2021 1decota.sydneyNo ratings yet
- 2D TransformationDocument38 pages2D TransformationSarvodhya Bahri0% (1)
- Civil Engineering Softwares and Their ImplementationsDocument13 pagesCivil Engineering Softwares and Their ImplementationsADITYANo ratings yet
- Generator Honda EP2500CX1Document50 pagesGenerator Honda EP2500CX1Syamsul Bahry HarahapNo ratings yet
- FisheryDocument2 pagesFisheryKyle GalangueNo ratings yet
- Soften, Soothe, AllowDocument1 pageSoften, Soothe, AllowTatiannaMartinsNo ratings yet
- Conference Flyer ChosenDocument4 pagesConference Flyer ChosenOluwatobi OgunfoworaNo ratings yet
- Channel Emotions into FlowDocument2 pagesChannel Emotions into Flowmaxalves77No ratings yet
- Tentech MTD20KWe Digital Earth Tester Users Guide ManualDocument45 pagesTentech MTD20KWe Digital Earth Tester Users Guide ManualAnonymous voVeDickM100% (1)
- How to introduce yourself in 60 secondsDocument15 pagesHow to introduce yourself in 60 secondsJaneGuinumtadNo ratings yet
- Let's think step by step:- The common factor of 32, 45 and 50 is 5- 32/5 = 6.4 meters - 45/5 = 9 meters- 50/5 = 10 meters- So the best option is the 50 meter wire.b. How did you get the answerDocument59 pagesLet's think step by step:- The common factor of 32, 45 and 50 is 5- 32/5 = 6.4 meters - 45/5 = 9 meters- 50/5 = 10 meters- So the best option is the 50 meter wire.b. How did you get the answerjsphmnsycjrscribdNo ratings yet
- 302340KWDocument22 pages302340KWValarmathiNo ratings yet
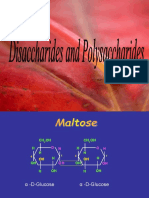
- Disaccharides and PolysaccharidesDocument17 pagesDisaccharides and PolysaccharidesAarthi shreeNo ratings yet
- Overcoming ChallengesDocument28 pagesOvercoming ChallengesDeutsche Mark CuynoNo ratings yet
- 06Document11 pages06junaid_ishaqueNo ratings yet
- Salary Survey (Hong Kong) - 2022Document7 pagesSalary Survey (Hong Kong) - 2022Nathan SmithNo ratings yet
- Units 3 - 4 Workshop A2Document3 pagesUnits 3 - 4 Workshop A2S4N7Y PRONo ratings yet
- General and Local AnesthesiaDocument1 pageGeneral and Local Anesthesiaahmedhelper300No ratings yet
- Ruibal & Shoemaker 1984 - Osteoders in AnuransDocument17 pagesRuibal & Shoemaker 1984 - Osteoders in AnuransRuivo LucasNo ratings yet
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Love Yourself, Heal Your Life Workbook (Insight Guide)From EverandLove Yourself, Heal Your Life Workbook (Insight Guide)Rating: 5 out of 5 stars5/5 (40)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)