You might also like
- Historical Recordings PDFDocument1 pageHistorical Recordings PDFbuendiainsideNo ratings yet
- Engagement in A Community-Based Integral Practice Program EnhanceDocument17 pagesEngagement in A Community-Based Integral Practice Program EnhancebuendiainsideNo ratings yet
- Blues Variations PDFDocument1 pageBlues Variations PDFbuendiainsideNo ratings yet
- Listenings PDFDocument1 pageListenings PDFbuendiainsideNo ratings yet
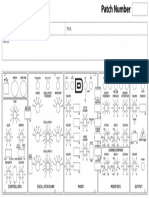
- Behringer Model D Patch SheetDocument1 pageBehringer Model D Patch SheetbuendiainsideNo ratings yet
- The Modes: ("Major", "Melodic Minor", "Harmonic Minor" & The "Harmonic Major" Modes)Document1 pageThe Modes: ("Major", "Melodic Minor", "Harmonic Minor" & The "Harmonic Major" Modes)buendiainsideNo ratings yet
- Major TriadsDocument10 pagesMajor Triadsbuendiainside100% (1)
- How To Manage One's Moods - The Book of LifeDocument8 pagesHow To Manage One's Moods - The Book of LifebuendiainsideNo ratings yet
- Update On Metabolism and Nutrition Therapy in Critically Ill Burned PatientsDocument11 pagesUpdate On Metabolism and Nutrition Therapy in Critically Ill Burned PatientsbuendiainsideNo ratings yet
- Nutritional Therapy in Major BurnsDocument6 pagesNutritional Therapy in Major BurnsRuth Danielle GasconNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Natural Eye CareDocument222 pagesNatural Eye Careskribdot100% (3)
- Lipid Metabolism - I: Chemistry, Digestion and Absorption of LipidsDocument38 pagesLipid Metabolism - I: Chemistry, Digestion and Absorption of LipidscheckmateNo ratings yet
- Detoxification GuideDocument29 pagesDetoxification GuideitorNo ratings yet
- KFC Grilled Chicken: Unthink Your HealthDocument10 pagesKFC Grilled Chicken: Unthink Your HealthNurul Safura RosliNo ratings yet
- Without Grain 100 Delicious Recipes For Eating A Grain-Free - Gluten-Free - Wheat-Free Diet PDFDocument211 pagesWithout Grain 100 Delicious Recipes For Eating A Grain-Free - Gluten-Free - Wheat-Free Diet PDFChuôngGió100% (1)
- Berardi Meal PlansDocument69 pagesBerardi Meal PlansJorge Alba Renedo100% (2)
- Sesame Oil Refined-Tx008267 PdsDocument3 pagesSesame Oil Refined-Tx008267 PdsAbdul Rahman ChoudhryNo ratings yet
- Diabetic Diet Plan: Quickstart GuideDocument166 pagesDiabetic Diet Plan: Quickstart GuideVirendra JoshiNo ratings yet
- Old Master Painting TechniqueDocument23 pagesOld Master Painting TechniqueChris Walker100% (2)
- The Cholestrol LieDocument4 pagesThe Cholestrol LieVijay Khanna100% (1)
- Brains Buildings in 12 WeeksDocument12 pagesBrains Buildings in 12 WeeksSyamsulNo ratings yet
- Effects of Omega-3 Fatty Acids On Lipids and Glycemic ControlDocument160 pagesEffects of Omega-3 Fatty Acids On Lipids and Glycemic ControlAndrzej SzymańskiNo ratings yet
- Amon409 415Document7 pagesAmon409 415MogleNo ratings yet
- Modern Diet Leads to Chronic DiseaseDocument11 pagesModern Diet Leads to Chronic DiseaseAldea VeganaNo ratings yet
- Experts' Findings On The Health Benefits of Coconut OilDocument2 pagesExperts' Findings On The Health Benefits of Coconut OilDuy AlphaNo ratings yet
- Black Seed Oil 1PSP-7047 - DOSS - ENDocument7 pagesBlack Seed Oil 1PSP-7047 - DOSS - ENSANo ratings yet
- Top 10 Foods To Increase MetabolismDocument4 pagesTop 10 Foods To Increase MetabolismGabriel CaraveteanuNo ratings yet
- Smart 2015 by Dave PalumboDocument116 pagesSmart 2015 by Dave PalumboВиктор Цонев-Каброне100% (16)
- Classification of Fats: Types by Composition, Fatty Acids, Requirement & SourcesDocument8 pagesClassification of Fats: Types by Composition, Fatty Acids, Requirement & Sourcesvovietphi123456No ratings yet
- 10 Cancer Fighting FoodsDocument5 pages10 Cancer Fighting FoodsNaushad AlamNo ratings yet
- Lipid Chemistry FST3107Document126 pagesLipid Chemistry FST3107ZHOU TIANLENo ratings yet
- SpirulinaDocument57 pagesSpirulinaMarcus Gibson100% (4)
- JJ Virgin Diet Shake BookletDocument16 pagesJJ Virgin Diet Shake Booklet224118100% (1)
- Linseed and Linseed Oil: Health Benefits-A Review: Vijaya Tripathi, A.B.Abidi, S. Marker, S.BilalDocument9 pagesLinseed and Linseed Oil: Health Benefits-A Review: Vijaya Tripathi, A.B.Abidi, S. Marker, S.BilalKrissa sunastiNo ratings yet
- Cargill VinodDocument98 pagesCargill Vinodsaurajindal09No ratings yet
- Da in OrderDocument28 pagesDa in Orderapi-282806729No ratings yet
- The Macronutrient: FATS: Laboratory Exercise No. 6Document7 pagesThe Macronutrient: FATS: Laboratory Exercise No. 6Maureen LeahNo ratings yet
- The Best Human Diet: 'Eat Food, Not Too Much, Mostly Plants'Document20 pagesThe Best Human Diet: 'Eat Food, Not Too Much, Mostly Plants'nyt100% (4)