You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- For The Candidates Admitted From The Academic Year 2013-2014 OnwardsDocument9 pagesFor The Candidates Admitted From The Academic Year 2013-2014 OnwardsPradeep PradyNo ratings yet
- For The Candidates Admitted From The Academic Year 2013-2014 OnwardsDocument9 pagesFor The Candidates Admitted From The Academic Year 2013-2014 OnwardsPradeep PradyNo ratings yet
- For The Candidates Admitted From The Academic Year 2013-2014 OnwardsDocument9 pagesFor The Candidates Admitted From The Academic Year 2013-2014 OnwardsPradeep PradyNo ratings yet
- Provisional Restorations: An Overview of Materials UsedDocument4 pagesProvisional Restorations: An Overview of Materials UsedPradeep PradyNo ratings yet
- 27 Posts of DCIO Final ScrutinyDocument2 pages27 Posts of DCIO Final ScrutinyPradeep PradyNo ratings yet
- A Technique For Impressing The Severely Resorbed MDocument5 pagesA Technique For Impressing The Severely Resorbed MPradeep Prady100% (1)
- ProsthodonticsDocument1 pageProsthodonticsPradeep PradyNo ratings yet
- The Finish Line: Sri Ramachandra Faculty of Dental SciencesDocument4 pagesThe Finish Line: Sri Ramachandra Faculty of Dental SciencesPradeep PradyNo ratings yet
- 88 JMSCRDocument4 pages88 JMSCRPradeep PradyNo ratings yet
- SJRD Id34Document5 pagesSJRD Id34Pradeep PradyNo ratings yet
- Zoom Phone Product Overview PDFDocument2 pagesZoom Phone Product Overview PDFPradeep PradyNo ratings yet
- Viva Questions OpDocument21 pagesViva Questions OpPradeep PradyNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Power Link Module For LD 800PDocument4 pagesPower Link Module For LD 800PSarah FrazierNo ratings yet
- Components and Nozzles: Job GuideDocument106 pagesComponents and Nozzles: Job GuideArtur TylickiNo ratings yet
- The Final War by Judge Rutherford, 1932Document65 pagesThe Final War by Judge Rutherford, 1932sirjsslutNo ratings yet
- BA JapanesePG PDFDocument7 pagesBA JapanesePG PDFIan IskandarNo ratings yet
- An Accurate DDS Method Using Compound Frequency Tuning Word and Its FPGA ImplementationDocument14 pagesAn Accurate DDS Method Using Compound Frequency Tuning Word and Its FPGA ImplementationKit CornNo ratings yet
- 2010-2004 Touch Up Paint CatalogDocument23 pages2010-2004 Touch Up Paint CatalogLucas WebbNo ratings yet
- Strategies For HarvestDocument86 pagesStrategies For HarvestBeka AsraNo ratings yet
- Engglis Isma E. N (18010107023) Tadris IpaDocument6 pagesEngglis Isma E. N (18010107023) Tadris IpaLita Dwi HasjayaNo ratings yet
- Highway EngineeringDocument27 pagesHighway EngineeringCari RedNo ratings yet
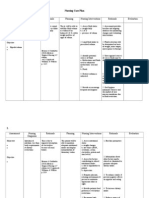
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- Immo Off FilesDocument6 pagesImmo Off Filesاليزيد بن توهامي100% (1)
- Layer 3 48-Port 10G SFP+ + 2-Port 40G QSFP+ + 4-Port 100G QSFP28 Managed SwitchDocument10 pagesLayer 3 48-Port 10G SFP+ + 2-Port 40G QSFP+ + 4-Port 100G QSFP28 Managed Switchbader eddine khezamiNo ratings yet
- Mummy The Curse Storytellers Vault Style Guide (With Bookmarks) 3 - 29 - 2019Document12 pagesMummy The Curse Storytellers Vault Style Guide (With Bookmarks) 3 - 29 - 2019Nick Iijima100% (2)
- Potential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334Document6 pagesPotential Targets For Antifungal Drug Discovery - Creative Biolabs - 1619624328334DicksonNo ratings yet
- Mimaki CJV-150 PDFDocument146 pagesMimaki CJV-150 PDFKisgyörgy ZoltánNo ratings yet
- Equation of Motion PDFDocument2 pagesEquation of Motion PDFMazvita TakawiraNo ratings yet
- JIS ThreadsDocument7 pagesJIS Threadsthailan0% (1)
- RmitDocument9 pagesRmitrajeevermaNo ratings yet
- Chinese Journal of Chemistry, 31 (1), 15-17 (2013) - DrospirenoneDocument3 pagesChinese Journal of Chemistry, 31 (1), 15-17 (2013) - DrospirenoneSam SonNo ratings yet
- Nutritional StatusDocument13 pagesNutritional StatusArlene ValenzuelaNo ratings yet
- ASME BPVC Section V (526-530)Document5 pagesASME BPVC Section V (526-530)Reza Elang HangkosoNo ratings yet
- Safety Data Sheet: 1. Identification of The Substance / Mixture and of The Company /undertakingDocument7 pagesSafety Data Sheet: 1. Identification of The Substance / Mixture and of The Company /undertakingOrshanetzNo ratings yet
- Presidential Theme: 66 Annual Conference of Indian Orthopaedic AssociationDocument16 pagesPresidential Theme: 66 Annual Conference of Indian Orthopaedic AssociationDr Jaspreet Singh0% (1)
- TEST SHEET139: 2021-2022: TERM: 1: Section B: Text AnalysisDocument2 pagesTEST SHEET139: 2021-2022: TERM: 1: Section B: Text AnalysisLavanya SharmaNo ratings yet
- Mashkoor Hussain Qureshi Ex PackagesDocument8 pagesMashkoor Hussain Qureshi Ex Packagesmussadaq raufNo ratings yet
- CARDIOPULMONARY BYPASS - CompressedDocument117 pagesCARDIOPULMONARY BYPASS - CompressedBayan TahaNo ratings yet
- Design of Aqueduct TroughDocument4 pagesDesign of Aqueduct TroughVinay Chandwani100% (1)
- Sourcing Report - Iffco Olive OilDocument13 pagesSourcing Report - Iffco Olive OilMatheusNo ratings yet
- Secondary Steering PumpDocument5 pagesSecondary Steering PumpStar SealNo ratings yet
- Use of Force ContinuumDocument1 pageUse of Force ContinuumNyloc100% (1)