You might also like
- Páginas Desdepharmacotherapy Casebook 10th Ed.Document61 pagesPáginas Desdepharmacotherapy Casebook 10th Ed.Glo VsNo ratings yet
- Biology Final Exam Grade 9Document2 pagesBiology Final Exam Grade 9Yesha Shah100% (1)
- Danish Mask StudyDocument1 pageDanish Mask StudyJuana AtkinsNo ratings yet
- Development & Growth Nutrition & Behavioral DisordersDocument27 pagesDevelopment & Growth Nutrition & Behavioral Disordershasanatiya41No ratings yet
- Constipation in ChildrenDocument17 pagesConstipation in ChildrenbellabelbonNo ratings yet
- Eating DisordersDocument15 pagesEating DisordersJana Marie CorpuzNo ratings yet
- Care of The Child With Gastrointestinal Dysfunction: Betsy Johnson, MSN, CPNP-PCDocument66 pagesCare of The Child With Gastrointestinal Dysfunction: Betsy Johnson, MSN, CPNP-PCGelsey Gelsinator JianNo ratings yet
- Pdf-Eating-Disorders Finals PDFDocument6 pagesPdf-Eating-Disorders Finals PDFVictor MurilloNo ratings yet
- Failure To Thrive: Premi Suresh, MD, FAAPDocument57 pagesFailure To Thrive: Premi Suresh, MD, FAAPsiti hazard aldinaNo ratings yet
- Eating DisordersDocument23 pagesEating Disordersipilham001No ratings yet
- Eating Disorders 101: Helpline: 800-931-2237 Business Line: 212-575-6200Document34 pagesEating Disorders 101: Helpline: 800-931-2237 Business Line: 212-575-6200uday kiranNo ratings yet
- Pertemuan 14 - Eating DisoredersDocument29 pagesPertemuan 14 - Eating Disoredersnada nabillaNo ratings yet
- NGRAbdominalComplaints5 16 12Document102 pagesNGRAbdominalComplaints5 16 12Timothy Eduard A. SupitNo ratings yet
- EpleyDocument51 pagesEpleyapi-536242116No ratings yet
- History Taking Clinical Examination in DiabetesDocument48 pagesHistory Taking Clinical Examination in DiabetesSanjeedha100% (1)
- FTT 4Document49 pagesFTT 4Pratita Jati PermatasariNo ratings yet
- Week 7 - Pediatric GI DisturbancesDocument59 pagesWeek 7 - Pediatric GI DisturbancesLeyla GalyanoNo ratings yet
- Pediatric Nutrition 2020 SGDocument27 pagesPediatric Nutrition 2020 SGHajira GhaniNo ratings yet
- PDF Ejemplos FRDocument6 pagesPDF Ejemplos FRConstanza MarinNo ratings yet
- Anorexia Nervosa and Anorexia BulimiaDocument3 pagesAnorexia Nervosa and Anorexia Bulimiainsta aNo ratings yet
- Hyperemesis GravidarumDocument16 pagesHyperemesis GravidarumGracy Casaña100% (2)
- Eating Disorders: Trisha IrelandDocument38 pagesEating Disorders: Trisha IrelandRegina PunNo ratings yet
- Psy240 Winter2024 Lecture6Document76 pagesPsy240 Winter2024 Lecture6aya.mazin99No ratings yet
- Protein Energy MalnutritionDocument33 pagesProtein Energy MalnutritionSarad Chand Yadav50% (2)
- 4Document3 pages4Moon KillerNo ratings yet
- Eating Disorders: Anorexia vs. BulimiaDocument17 pagesEating Disorders: Anorexia vs. BulimiabajaocNo ratings yet
- Eatng DisordersDocument28 pagesEatng DisordersRupinder GillNo ratings yet
- Protein Energy MalnutritionDocument133 pagesProtein Energy MalnutritionMuhammad Anas AbbalNo ratings yet
- Persistent Diarrhoea & Chronic DiarrhoeaDocument34 pagesPersistent Diarrhoea & Chronic DiarrhoeanilmbbsNo ratings yet
- Anorexia Nervosa: Dr. K.RavishankarDocument17 pagesAnorexia Nervosa: Dr. K.RavishankarChaitanya Kiran PullelaNo ratings yet
- PSM ExaminationDocument5 pagesPSM ExaminationRoshan KumarNo ratings yet
- Efek Eating Disorder Terhadap Remaja: Nindy Sabrina, S.GZ, M.SCDocument22 pagesEfek Eating Disorder Terhadap Remaja: Nindy Sabrina, S.GZ, M.SClulukNo ratings yet
- Psychiatric Mental Health CareDocument11 pagesPsychiatric Mental Health CareAmir PermitivoNo ratings yet
- This Is A Awarreness Poster Made by Harsh Vagal About The Eating Disorders Namely Bulimia/anorexia Nervosa and ObesityDocument2 pagesThis Is A Awarreness Poster Made by Harsh Vagal About The Eating Disorders Namely Bulimia/anorexia Nervosa and ObesityHarsh VagalNo ratings yet
- NUT202: Fundamentals of Human Nutrition: Chapter 6: Eating DisordersDocument49 pagesNUT202: Fundamentals of Human Nutrition: Chapter 6: Eating DisordersGhina RedaNo ratings yet
- Common Health Problems That Develop During InfancyDocument28 pagesCommon Health Problems That Develop During Infancylaurie.charlynjaneNo ratings yet
- Nutrition & Diet Therapy: Carbohydrate-Modified Diets For DiabetesDocument25 pagesNutrition & Diet Therapy: Carbohydrate-Modified Diets For Diabetescatu11100% (1)
- Anorexia Vs BulimiaDocument19 pagesAnorexia Vs BulimiaNylia AtibiNo ratings yet
- 62 DiarrheaChronic MGHG MIMG MFM 20161229Document10 pages62 DiarrheaChronic MGHG MIMG MFM 20161229Wei HangNo ratings yet
- Refluxver 23Document31 pagesRefluxver 23Osman Bin SaifNo ratings yet
- History Taking Git: Dr. Sofi MD FRCP (London) Frcpedin FrcsedinDocument23 pagesHistory Taking Git: Dr. Sofi MD FRCP (London) Frcpedin FrcsedinusamaNo ratings yet
- Nutritional Assesment: Group 3 Fefrina Helda Rany Ika Fardila Ridho Mahendra Zahara Muthia RusdyDocument30 pagesNutritional Assesment: Group 3 Fefrina Helda Rany Ika Fardila Ridho Mahendra Zahara Muthia RusdyNadia MulyaNo ratings yet
- Eating DisordersDocument36 pagesEating Disordersclarence_parales100% (1)
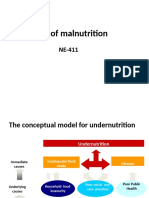
- Causes of MalnutritionDocument13 pagesCauses of MalnutritionEman ZahraNo ratings yet
- Feeding Presentation South Africa 1Document141 pagesFeeding Presentation South Africa 1Fouzia IdreesNo ratings yet
- ISCP 4th Hari Kedua GoodDocument72 pagesISCP 4th Hari Kedua GoodMade SriNo ratings yet
- Elective Course "Public Health Aspect of Childhood Diseases: Slides Focused On Questions From The TestDocument37 pagesElective Course "Public Health Aspect of Childhood Diseases: Slides Focused On Questions From The TestAki QkoelNo ratings yet
- Cerebral PalsyDocument96 pagesCerebral PalsyRahini PaniNo ratings yet
- R Eating DisordersDocument33 pagesR Eating DisordersFev BanataoNo ratings yet
- Prader-Willi SyndromeDocument45 pagesPrader-Willi Syndromeapi-554351240No ratings yet
- Eating DisordersDocument43 pagesEating DisordersMary Margarett Boado0% (1)
- Gastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsDocument77 pagesGastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsSindhu BabuNo ratings yet
- AnxietyDocument51 pagesAnxietydivyaNo ratings yet
- DiarrhoeaDocument33 pagesDiarrhoeasandhyaa7srinivassanNo ratings yet
- Eating DisordersDocument37 pagesEating DisordersReeycha ShresthaNo ratings yet
- Eating Disorders: Dr. Shastri MotilalDocument26 pagesEating Disorders: Dr. Shastri MotilalSaraNo ratings yet
- Weight-Related Concerns and Disorders Among Adolescents: PKK 3203 Nutrition Throughout The Life CycleDocument48 pagesWeight-Related Concerns and Disorders Among Adolescents: PKK 3203 Nutrition Throughout The Life Cyclechen chendaeNo ratings yet
- Chapter 020Document33 pagesChapter 020api-3697326No ratings yet
- Nutrition and DieteticsDocument53 pagesNutrition and DieteticsLouie ParillaNo ratings yet
- Protein Energy MalnutritionDocument44 pagesProtein Energy Malnutritionokwadha simionNo ratings yet
- Pir Refeeding PPT FinalDocument13 pagesPir Refeeding PPT FinalbentoeNo ratings yet
- Vegetative DisordersDocument55 pagesVegetative DisordersAnil NarayanNo ratings yet
- Handbook of Clinical SkillsDocument56 pagesHandbook of Clinical SkillsRamadan MustafaNo ratings yet
- Basics of EKG InterpretationDocument132 pagesBasics of EKG InterpretationArif Imam HidayatNo ratings yet
- Pelvis 1stpartDocument36 pagesPelvis 1stpartRamadan MustafaNo ratings yet
- AnginaDocument16 pagesAnginaRamadan MustafaNo ratings yet
- MEdication ErrorsDocument6 pagesMEdication ErrorsBeaCeeNo ratings yet
- Hemostat Thromboplastin-SI: Determination of Prothrombin Time (PT)Document2 pagesHemostat Thromboplastin-SI: Determination of Prothrombin Time (PT)Lemi MaluluNo ratings yet
- The Terrorist Inside My Husband's Brain PDFDocument5 pagesThe Terrorist Inside My Husband's Brain PDFraymondnomyarNo ratings yet
- 83 Nutripuncture OverviewDocument12 pages83 Nutripuncture OverviewTimoteo Pereira TfmpNo ratings yet
- Pes Planus Concept MapDocument2 pagesPes Planus Concept MapVeronica Jean U. TubaonNo ratings yet
- Eating Disorders Eating Disorders OverviewDocument12 pagesEating Disorders Eating Disorders OverviewGiancarlo CrespoNo ratings yet
- ABC Quality and Patient Saftey Workshop FinalDocument68 pagesABC Quality and Patient Saftey Workshop Finalyousrazeidan1979No ratings yet
- The Ivf Pack 2 PDFDocument11 pagesThe Ivf Pack 2 PDFPaula BošnjakNo ratings yet
- Onco-Critical Care An Evidence-Based ApproachDocument539 pagesOnco-Critical Care An Evidence-Based ApproachZuriNo ratings yet
- PRN Effectiveness PresentationDocument14 pagesPRN Effectiveness Presentationapi-457177638No ratings yet
- Reffered PainDocument26 pagesReffered PainHappy Septianto SNo ratings yet
- Steroids Other Appearance Performance Enhancing Drugs Apeds Research ReportDocument34 pagesSteroids Other Appearance Performance Enhancing Drugs Apeds Research ReportFit and LiftNo ratings yet
- Coexistence of Papillary Carcinoma and Hashimoto S ThyroiditisDocument4 pagesCoexistence of Papillary Carcinoma and Hashimoto S Thyroiditispooo80No ratings yet
- Twin Block 3Document2 pagesTwin Block 3GisselaMaldonadoNo ratings yet
- Arihant Hospital & Research CentreDocument30 pagesArihant Hospital & Research CentreSourabhSharmaNo ratings yet
- MHC PDFDocument2 pagesMHC PDFYuvarani AruchamyNo ratings yet
- Komunikasi Asuhan Pasien - KARS - 2019Document93 pagesKomunikasi Asuhan Pasien - KARS - 2019Yudi Tubagja SiregarNo ratings yet
- Nursing Care Plan Guide: Subjective DataDocument1 pageNursing Care Plan Guide: Subjective DataJan Oliver YaresNo ratings yet
- Senior CapstoneDocument6 pagesSenior Capstoneapi-313278667No ratings yet
- Esophageal SpasmDocument11 pagesEsophageal SpasmHafidz RosliNo ratings yet
- Patient Delivery Receipt: Product Delivery Location: FacilityDocument1 pagePatient Delivery Receipt: Product Delivery Location: FacilityPat Dela CruzNo ratings yet
- 3in1 Shoulder BlockDocument2 pages3in1 Shoulder BlockTejasvi ChandranNo ratings yet
- Continue Renal Replacement Therapy: 1. CVVH 2. CVVHD 3. CVVHDFDocument21 pagesContinue Renal Replacement Therapy: 1. CVVH 2. CVVHD 3. CVVHDFhengki jokteryNo ratings yet
- Revitears Study 2Document16 pagesRevitears Study 2office.hospimedNo ratings yet
- EXERCISE Stress Testing FOR HEARTDocument52 pagesEXERCISE Stress Testing FOR HEARTBenjamin GonzalezNo ratings yet
- The Effect of Mangosteen (Garcinia Mangostana) Rind in The Blood Glucose Levels of Adult Patients With Type 2 Diabetes MellitusDocument4 pagesThe Effect of Mangosteen (Garcinia Mangostana) Rind in The Blood Glucose Levels of Adult Patients With Type 2 Diabetes MellitusFiqoh Puteri FauziNo ratings yet
- CKD + HPN Concept Map DRAFTDocument1 pageCKD + HPN Concept Map DRAFTInah Floresta BesasNo ratings yet