You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- High Yield PediatricsDocument78 pagesHigh Yield Pediatricsjose100% (1)
- DryDock CompleteDocument24 pagesDryDock Completeashry_tarek100% (2)
- Drill String Design 4.11Document23 pagesDrill String Design 4.11Ryan Tan Ping Yi100% (1)
- Example of Fraudulent MachinationsDocument2 pagesExample of Fraudulent MachinationsJvnRodz P Gmlm100% (4)
- Facility Management Plan (FMP) Facilities Health, Safety & Environmental (Hse) ManagementDocument35 pagesFacility Management Plan (FMP) Facilities Health, Safety & Environmental (Hse) ManagementAhmad Saiful Ridzwan Jaharuddin100% (2)
- PSA GeneralDocument17 pagesPSA GeneralMohammed AhmedNo ratings yet
- Selection of Separator With BootDocument2 pagesSelection of Separator With BootMaryJane Ayisha Sado-ObahNo ratings yet
- MS Road Marking & Furniture - DRAFTDocument16 pagesMS Road Marking & Furniture - DRAFTfadhilahNo ratings yet
- Answer Key Grade Six: Weathering and Erosion: Multiple Choice: (4 Points Each)Document5 pagesAnswer Key Grade Six: Weathering and Erosion: Multiple Choice: (4 Points Each)emmanuel richardNo ratings yet
- Sworn Statement of Assets, Liabilities and Net Worth: Joint Filing Separate Filing Not ApplicableDocument4 pagesSworn Statement of Assets, Liabilities and Net Worth: Joint Filing Separate Filing Not ApplicableTheoSebastianNo ratings yet
- Trial 2017 MRSM p3 Answer Scheme BioDocument9 pagesTrial 2017 MRSM p3 Answer Scheme Biolittle princessNo ratings yet
- Foundation Harmony ATC ApplicationDocument85 pagesFoundation Harmony ATC ApplicationNew Jersey marijuana documentsNo ratings yet
- MSDS ProkleenDocument6 pagesMSDS ProkleenDesta Eka PrasetyaNo ratings yet
- 1 Land Rover Freelander MY2001 Parking Heater Install TD4Document4 pages1 Land Rover Freelander MY2001 Parking Heater Install TD4Florin ConstantinNo ratings yet
- Battery Fuses Megane 2Document18 pagesBattery Fuses Megane 2osdasoNo ratings yet
- The Effect of The Cementitious Paste Thickness On The Performance of Pervious ConcreteDocument10 pagesThe Effect of The Cementitious Paste Thickness On The Performance of Pervious ConcreteEverton RenatoNo ratings yet
- Granda-Ramírez2017 Article DegradationOfRecalcitrantSafraDocument12 pagesGranda-Ramírez2017 Article DegradationOfRecalcitrantSafraLeidy StefanyNo ratings yet
- ENGLISH III - ACTIVITY 7 - DanielDocument2 pagesENGLISH III - ACTIVITY 7 - DanielDaniel David GutierrezNo ratings yet
- 11.8 Chemical Equilibrium Solution - PremiumDocument20 pages11.8 Chemical Equilibrium Solution - PremiumJonathan ParkerNo ratings yet
- BSM Admissions Application-FormDocument5 pagesBSM Admissions Application-Formeliesha rejiNo ratings yet
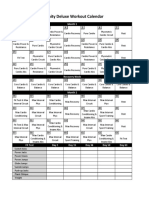
- Insanity Workout Deluxe Calendar SimpleDocument1 pageInsanity Workout Deluxe Calendar SimpleCristian Manuel GonzálezNo ratings yet
- HematologyDocument100 pagesHematologyerzaraptorNo ratings yet
- Caalogo Allen BradleyDocument27 pagesCaalogo Allen BradleyricardoqqNo ratings yet
- Mineral Resources and Food ResourcesDocument31 pagesMineral Resources and Food Resourcesvaishali TMU studentNo ratings yet
- Social Exclusion: Towards A Holistic Understanding of DeprivationDocument22 pagesSocial Exclusion: Towards A Holistic Understanding of DeprivationDaniel MedeirosNo ratings yet
- Per Section Contests A. Poster Making Contest MechanicsDocument4 pagesPer Section Contests A. Poster Making Contest MechanicsMaribel Dizon MangioNo ratings yet
- Chap 37Document13 pagesChap 37buatadekNo ratings yet
- Carvera Manual EngDocument30 pagesCarvera Manual EngBilly DipperNo ratings yet
- Sensor HardwareDocument34 pagesSensor HardwareLoya SrijaNo ratings yet
- AmbergrisDocument4 pagesAmbergriskaram deolNo ratings yet