You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- dlm12l Laboratory-CentrifugeDocument50 pagesdlm12l Laboratory-Centrifugehüseyin vururNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Abortion Op EdDocument3 pagesAbortion Op EdMadeline GlotfeltyNo ratings yet
- Ginseng Qianjin Yi FangDocument3 pagesGinseng Qianjin Yi FangRobert A. ThrelfallNo ratings yet
- The Immune System in Health and DiseaseDocument30 pagesThe Immune System in Health and DiseaseApshar Munna100% (1)
- Safety and Reference: Owner'S ManualDocument40 pagesSafety and Reference: Owner'S ManualRaj ThakurNo ratings yet
- Arun Ice Cream Strategic Management Case StudyDocument18 pagesArun Ice Cream Strategic Management Case Studyvar18111989100% (1)
- CHEM 121 - General Chemistry Chapter 1Document14 pagesCHEM 121 - General Chemistry Chapter 1kingdom12828No ratings yet
- Sonar: Firestone (1940) and Simons (1945)Document9 pagesSonar: Firestone (1940) and Simons (1945)Tom JonesNo ratings yet
- Traditional and Modern Self OutlookDocument3 pagesTraditional and Modern Self Outlookethan philasia90% (10)
- Organizational Development Case Analysis-The Old Family BankDocument3 pagesOrganizational Development Case Analysis-The Old Family BankFabian HartmannNo ratings yet
- CE 111 Quiz 1 August 2012Document2 pagesCE 111 Quiz 1 August 2012AJ SaNo ratings yet
- The Mental Health Status of Grade 11 ABM Students During The Online Learning Set Up in Davao CityDocument19 pagesThe Mental Health Status of Grade 11 ABM Students During The Online Learning Set Up in Davao CityALYANNA SARMIENTONo ratings yet
- FAW ScriptDocument6 pagesFAW ScriptKVK East Khasi hillsNo ratings yet
- Nama: No. CM: Ruangan:: Formulir Potensi KegawatanDocument3 pagesNama: No. CM: Ruangan:: Formulir Potensi KegawatanriniNo ratings yet
- Urine Preservatives-Collection and Transportation For 24-Hour Urine SpecimensDocument5 pagesUrine Preservatives-Collection and Transportation For 24-Hour Urine SpecimensFaryalBalochNo ratings yet
- 218 JAMBA DPversion1Document7 pages218 JAMBA DPversion1Shirley Jean Villamor SuganoNo ratings yet
- Arlegui Seminar RoomDocument1 pageArlegui Seminar RoomGEMMA PEPITONo ratings yet
- The World 07232014Document36 pagesThe World 07232014The WorldNo ratings yet
- Sewage Disposal 19 03 17Document6 pagesSewage Disposal 19 03 17Vikash ChoudharyNo ratings yet
- 001 Pharmacognostical and Physicochemical Characteristics of Roots of Lesser Known Medicinal Plant Caesalpinia Digyna PDFDocument5 pages001 Pharmacognostical and Physicochemical Characteristics of Roots of Lesser Known Medicinal Plant Caesalpinia Digyna PDFKannanNo ratings yet
- Electricity Generation Cost Report 2020Document72 pagesElectricity Generation Cost Report 2020Sanuwar RahmanNo ratings yet
- Marstall Katalog-English WEBDocument80 pagesMarstall Katalog-English WEBeovidiuNo ratings yet
- A Typical Synovial JointDocument8 pagesA Typical Synovial JointSheena Mae AtienzaNo ratings yet
- ITPDocument27 pagesITPYosuaNo ratings yet
- St. Anthony's College Nursing Department San Jose, AntiqueDocument30 pagesSt. Anthony's College Nursing Department San Jose, AntiqueTweenie DalumpinesNo ratings yet
- Kendriya Vidyalaya Sambalpur: Science Project SESSION 2016-17 Topic-Fishes Pujarani Behera Ix - C 16 S.S.Bhoi SirDocument8 pagesKendriya Vidyalaya Sambalpur: Science Project SESSION 2016-17 Topic-Fishes Pujarani Behera Ix - C 16 S.S.Bhoi SirNiranjan BeheraNo ratings yet
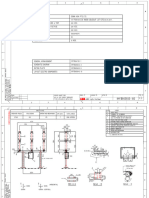
- Drawing CB LTB 145D1 - BDocument9 pagesDrawing CB LTB 145D1 - Btoàn lêNo ratings yet
- Pump Curve and DefinitionDocument8 pagesPump Curve and DefinitionAleidinNo ratings yet
- AS-7M108-HC Black Module Specification 1722-1134-30mmDocument2 pagesAS-7M108-HC Black Module Specification 1722-1134-30mmAlexandru GrosNo ratings yet