You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Clinical Pharmacy - Simple Notes PDFDocument186 pagesClinical Pharmacy - Simple Notes PDFsmart hussain86% (79)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Michael E. Aulton, Kevin M.G. Taylor - Aulton's Pharmaceutics - The Design and Manufacture of Medicines-Elsevier (2017) PDFDocument933 pagesMichael E. Aulton, Kevin M.G. Taylor - Aulton's Pharmaceutics - The Design and Manufacture of Medicines-Elsevier (2017) PDFsamanta100% (2)
- Module 3 Practice ProblemsDocument11 pagesModule 3 Practice ProblemsAli Veer Ali Veer0% (1)
- LIBRO NEURO UCI 2013 Monitoring in Neurocritical CareDocument602 pagesLIBRO NEURO UCI 2013 Monitoring in Neurocritical CareDiana Reaño RuizNo ratings yet
- Root Cause Analysis and Failure Mode and Effects AnalysisDocument56 pagesRoot Cause Analysis and Failure Mode and Effects AnalysisGokul100% (2)
- Toxicology and TDMDocument121 pagesToxicology and TDMteppie0917No ratings yet
- Math FINAL Study GuideDocument11 pagesMath FINAL Study GuideAnonymous 4Ajc32DZNo ratings yet
- Tugas MedicineDocument2 pagesTugas MedicineRiza Ikhsan MuliaNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument23 pagesEVMS Critical Care COVID-19 ProtocoldarwinNo ratings yet
- Nclex PogiDocument8 pagesNclex Pogijackyd5No ratings yet
- Prado, Catherine BSN IIB (Activity 1 Case Scenario)Document52 pagesPrado, Catherine BSN IIB (Activity 1 Case Scenario)Catherine PradoNo ratings yet
- Rome Alexander Culaton - Infomercial About Prevention Control of Substance Use Abuse Develop Resistance SkillsDocument2 pagesRome Alexander Culaton - Infomercial About Prevention Control of Substance Use Abuse Develop Resistance Skills레이reiNo ratings yet
- Zoloft SertralineDocument1 pageZoloft SertralineAdrianne Bazo100% (1)
- Standard Treatment Guidelines Sangeeta PDFDocument712 pagesStandard Treatment Guidelines Sangeeta PDFIosub Lica-Claudiu100% (4)
- TDM335782 111022101613 InvoiceDocument1 pageTDM335782 111022101613 InvoiceBalayya PattapuNo ratings yet
- Smart Drugs - Improving Healthcare Using Smart Pill Box For MedicinDocument15 pagesSmart Drugs - Improving Healthcare Using Smart Pill Box For MedicinLê Văn LưuNo ratings yet
- Chlorotoluene HPDocument71 pagesChlorotoluene HPShailesh LahotiNo ratings yet
- 421 Reproduction Developmental Toxicity Screening TestDocument10 pages421 Reproduction Developmental Toxicity Screening TestAshishNo ratings yet
- Snop SisDocument37 pagesSnop SisDr Sheetal kopardeNo ratings yet
- Types of Tablets and Their CharecteristicsDocument49 pagesTypes of Tablets and Their CharecteristicsRohit IrkalNo ratings yet
- HydrocortisoneDocument4 pagesHydrocortisonejoanah rose riveraNo ratings yet
- Medisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25DDocument2 pagesMedisiddh Pharma Private Limited 971A/6, Thirumal Nagar, Near K.R Arts College-Nh7, Kovilpatti-628503 LICENSE NO: 490/25Dhk_scribdNo ratings yet
- Effecto Pranayama Rechaka Puraka and Kumbaka On Bronchialasthma-Anopenstudy-3Document5 pagesEffecto Pranayama Rechaka Puraka and Kumbaka On Bronchialasthma-Anopenstudy-3Martina Pedreros RodríguezNo ratings yet
- Sirolimus ARCDocument9 pagesSirolimus ARCtesteste testeNo ratings yet
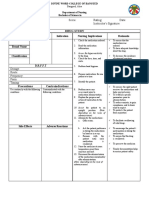
- Drug Study NCP Template 2Document2 pagesDrug Study NCP Template 2Janico Lanz BernalNo ratings yet
- Uniformity of Dosage UnitsDocument5 pagesUniformity of Dosage UnitsJai MurugeshNo ratings yet
- S 000 LBLDocument14 pagesS 000 LBLfaisal abbasNo ratings yet
- Administration of MedicationDocument10 pagesAdministration of MedicationYeesha Palacio BalmesNo ratings yet
- Guaifenesin Sample Package InsertDocument2 pagesGuaifenesin Sample Package InsertCyNo ratings yet
- Administration of MedicationsDocument11 pagesAdministration of MedicationsAsma Saleem100% (1)