You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grade 8 BowDocument7 pagesGrade 8 BowJorely Barbero MundaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- MCQ On PCR (Polymerase Chain Reaction) - MCQ Biology - Learning Biology Through MCQsDocument6 pagesMCQ On PCR (Polymerase Chain Reaction) - MCQ Biology - Learning Biology Through MCQsPpa Gpat Amit100% (2)
- Multiple Choice Questions On DNA Extraction - MCQ Biology - Learning Biology Through MCQsDocument5 pagesMultiple Choice Questions On DNA Extraction - MCQ Biology - Learning Biology Through MCQsPpa Gpat AmitNo ratings yet
- NCP For PoisoningDocument2 pagesNCP For PoisoningLorie Yvonne Quibin Agullana100% (1)
- MCQ On Animal Biotechnology - MCQ Biology - Learning Biology Through MCQsDocument5 pagesMCQ On Animal Biotechnology - MCQ Biology - Learning Biology Through MCQsPpa Gpat AmitNo ratings yet
- MCQ On Recombinant DNA Technology - MCQ Biology - Learning Biology Through MCQsDocument6 pagesMCQ On Recombinant DNA Technology - MCQ Biology - Learning Biology Through MCQsPpa Gpat AmitNo ratings yet
- Strengthening Mental Health and Psychosocial Support Systems and ServicesDocument116 pagesStrengthening Mental Health and Psychosocial Support Systems and ServicesPan PanNo ratings yet
- Pka TablesDocument39 pagesPka TablesRisa R.No ratings yet
- 6 2 1 2 Liquid-Preparations-For-Oral-Use PDFDocument4 pages6 2 1 2 Liquid-Preparations-For-Oral-Use PDFPpa Gpat AmitNo ratings yet
- Renin-Angio Sys-1Document27 pagesRenin-Angio Sys-1Ppa Gpat AmitNo ratings yet
- TLC PDFDocument33 pagesTLC PDFPpa Gpat AmitNo ratings yet
- s41568 018 0061 0 PDFDocument13 pagess41568 018 0061 0 PDFPpa Gpat AmitNo ratings yet
- 8 3 81 640 PDFDocument12 pages8 3 81 640 PDFPpa Gpat AmitNo ratings yet
- 6 2 1 5 Parenteral-Preparations PDFDocument4 pages6 2 1 5 Parenteral-Preparations PDFshaikNo ratings yet
- Thinlayerchromatography 150107132824 Conversion Gate02 PDFDocument107 pagesThinlayerchromatography 150107132824 Conversion Gate02 PDFPpa Gpat AmitNo ratings yet
- Suspension TestDocument37 pagesSuspension TestTerence EdayNo ratings yet
- 14 PDFDocument6 pages14 PDFPpa Gpat AmitNo ratings yet
- Chemical Shift and TMS PDFDocument2 pagesChemical Shift and TMS PDFPpa Gpat AmitNo ratings yet
- Skeletalmusclerelaxants 161103031625Document30 pagesSkeletalmusclerelaxants 161103031625Ppa Gpat AmitNo ratings yet
- Crack Gpat - 2020Document18 pagesCrack Gpat - 2020Tarun GuruvelliNo ratings yet
- Sterilization 171208105248 PDFDocument27 pagesSterilization 171208105248 PDFPpa Gpat AmitNo ratings yet
- Skeletalmusclerelaxants 161103031625Document30 pagesSkeletalmusclerelaxants 161103031625Ppa Gpat AmitNo ratings yet
- Sterilizationmethodsofparenterals 151124041956 Lva1 App6891 PDFDocument42 pagesSterilizationmethodsofparenterals 151124041956 Lva1 App6891 PDFPpa Gpat AmitNo ratings yet
- Woodward-Fieser UV Absorption RulesDocument1 pageWoodward-Fieser UV Absorption RulesPpa Gpat AmitNo ratings yet
- Taniyahplcseminar 150518175426 Lva1 App6892Document22 pagesTaniyahplcseminar 150518175426 Lva1 App6892Ppa Gpat AmitNo ratings yet
- Module-1 (MCQS) Fermentation-An IntroductionDocument2 pagesModule-1 (MCQS) Fermentation-An IntroductionPpa Gpat Amit0% (1)
- 14drugsactingonrespiratorysystem Expectorantsrespiratorystimulants 140109023212 Phpapp01Document19 pages14drugsactingonrespiratorysystem Expectorantsrespiratorystimulants 140109023212 Phpapp01Ppa Gpat AmitNo ratings yet
- Poison 180519043603Document106 pagesPoison 180519043603Ppa Gpat AmitNo ratings yet
- Our Success StoriesDocument9 pagesOur Success StoriesPpa Gpat AmitNo ratings yet
- Neem Tree: A Comprehensive Guide to its Uses, Benefits and HistoryDocument10 pagesNeem Tree: A Comprehensive Guide to its Uses, Benefits and Historyom prakashNo ratings yet
- J Semcancer 2018 05 001 PDFDocument41 pagesJ Semcancer 2018 05 001 PDFPpa Gpat AmitNo ratings yet
- Crack Gpat - 2020Document18 pagesCrack Gpat - 2020Tarun GuruvelliNo ratings yet
- HR Selection Process & Global PerspectivesDocument30 pagesHR Selection Process & Global PerspectivesOsei Kwame PhilipNo ratings yet
- Sop Saad 3Document2 pagesSop Saad 3ZarmeenaGauharNo ratings yet
- Clinical Reasoning Evaluation Simulation Tool (CREST)Document3 pagesClinical Reasoning Evaluation Simulation Tool (CREST)BenToNo ratings yet
- ProteinDocument89 pagesProteinAki OtaniNo ratings yet
- NCM 103 Administering Intramuscular MedicationDocument16 pagesNCM 103 Administering Intramuscular MedicationAdrynnette Cruz-LastimadoNo ratings yet
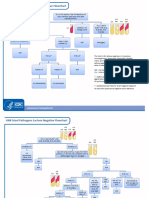
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- HTTPS: - Dacemirror - Sci-Hub - TW - Journal-Article - Soares2017 PDFDocument10 pagesHTTPS: - Dacemirror - Sci-Hub - TW - Journal-Article - Soares2017 PDFdarinsafinazNo ratings yet
- Maharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListDocument30 pagesMaharashtra Government PGM Admissions 2015-2016 Round 2 Selection ListAbhinav BhardwajNo ratings yet
- Johnson 2020 IOP Conf. Ser. Mater. Sci. Eng. 993 012022Document13 pagesJohnson 2020 IOP Conf. Ser. Mater. Sci. Eng. 993 012022astrid abigail blas sanchezNo ratings yet
- Effects of A Capacitive-Resistive Electric Transfer Therapy OnDocument8 pagesEffects of A Capacitive-Resistive Electric Transfer Therapy OnAnna Lygia LunardiNo ratings yet
- List of Visiting DoctorDocument3 pagesList of Visiting Doctordulal pramanickNo ratings yet
- 175 Hys, Matuszek, Olejnik, BierczyńskiDocument9 pages175 Hys, Matuszek, Olejnik, BierczyńskiRadek PolonusNo ratings yet
- Distraction Techniques For Face and Smile Aesthetic Preventing Ageing DecayDocument10 pagesDistraction Techniques For Face and Smile Aesthetic Preventing Ageing DecayAarónNo ratings yet
- Recruitment MSCDocument40 pagesRecruitment MSCViji MNo ratings yet
- Health Promotion On Nutrition For Children Under FiveDocument21 pagesHealth Promotion On Nutrition For Children Under FiveSinta WuLandariNo ratings yet
- UntitledDocument7 pagesUntitledSucdi AbdirazakNo ratings yet
- Session 1 - Listening HWDocument3 pagesSession 1 - Listening HWAnh N. NguyenNo ratings yet
- Vijaya Diagnostic HIV Test ReportDocument1 pageVijaya Diagnostic HIV Test Reportpasham bharat simha reddy100% (1)
- Therapeutic Communication: Emilio Aguinaldo CollegeDocument13 pagesTherapeutic Communication: Emilio Aguinaldo CollegeJor GarciaNo ratings yet
- Tool Box Talk - MK - Emergency Response ProceduresDocument2 pagesTool Box Talk - MK - Emergency Response ProceduresPaul McGahanNo ratings yet
- Introduction To Architectural ProgrammingDocument34 pagesIntroduction To Architectural ProgrammingbalaNo ratings yet
- Research Titles For DefenseDocument11 pagesResearch Titles For DefenseBelle Lee100% (1)
- HACH LANGE Ascorbic Acid PP (1457799) - ENGDocument5 pagesHACH LANGE Ascorbic Acid PP (1457799) - ENGkerem__22No ratings yet
- Pengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Document16 pagesPengumuman Jadwal Rapid Test Antigen Gratis Bagi Peserta Ujian SKB CPNS Pemerintah Kota Pangkalpinang 2021Syahrul SalehNo ratings yet
- English Assignment Direct and Indirect SentencesDocument6 pagesEnglish Assignment Direct and Indirect SentencesSasmita Novalis ArrizqiNo ratings yet
- Approach To Child With Headache: Dr. Vijaya Kumar Chikanbanjar 2nd Year Resident Department of PediatricsDocument49 pagesApproach To Child With Headache: Dr. Vijaya Kumar Chikanbanjar 2nd Year Resident Department of Pediatricsar bindraNo ratings yet
- What Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasDocument24 pagesWhat Is Criminal Rehabilitation?: Lisa Forsberg Thomas DouglasAisa VenturaNo ratings yet