You might also like
- Pictures You Need For SMLE EXAM by DR - Qasem PDFDocument9 pagesPictures You Need For SMLE EXAM by DR - Qasem PDFM ANo ratings yet
- Affidavit Complaint LanderoDocument4 pagesAffidavit Complaint LanderoUndo ValenzuelaNo ratings yet
- Theories of AgeingDocument6 pagesTheories of Ageingprince100% (1)
- Mental Health ActDocument8 pagesMental Health ActRaven Claire MalacaNo ratings yet
- National Structural Concrete SpecificationDocument77 pagesNational Structural Concrete SpecificationNana IbrahimNo ratings yet
- 3.shutter Island Movie AnylysisDocument33 pages3.shutter Island Movie AnylysisyashNo ratings yet
- Psychia Program Design GROUP2Document2 pagesPsychia Program Design GROUP2Pia Mae BuayaNo ratings yet
- Resume Safety ManagerDocument2 pagesResume Safety ManagerZied AbdelhediNo ratings yet
- Group 1 Mental Status ExaminationDocument12 pagesGroup 1 Mental Status ExaminationPankaj100% (2)
- Background On Mental HealthDocument10 pagesBackground On Mental HealthAmor GarciaNo ratings yet
- OACPA's Letter of Appeal To VERA Files Nov 18, 2022Document3 pagesOACPA's Letter of Appeal To VERA Files Nov 18, 2022VERA FilesNo ratings yet
- A Case Study of Mental DisorderDocument22 pagesA Case Study of Mental Disorderhershey100% (1)
- Pcol Lab Activity 2 3ADocument6 pagesPcol Lab Activity 2 3AMeryl Ann Ibarra-InganNo ratings yet
- RED BOOK - Full - Download - 01c5 PDFDocument252 pagesRED BOOK - Full - Download - 01c5 PDFDaniel Castro0% (1)
- Ka Leody de Guzman - Walden Bello PlatformDocument3 pagesKa Leody de Guzman - Walden Bello PlatformVERA FilesNo ratings yet
- The Evolution of Psychiatry and Mental Health in The PhilippinesDocument14 pagesThe Evolution of Psychiatry and Mental Health in The PhilippinesPaula Manalo-SuliguinNo ratings yet
- Bipolar I Disorder - CASE STUDYDocument62 pagesBipolar I Disorder - CASE STUDYJoy-Rena Sabinay OchondraNo ratings yet
- Mental Health Care of The PhilDocument4 pagesMental Health Care of The Philvenxel bantilanNo ratings yet
- DSM Iv TRDocument1 pageDSM Iv TRJehannah Dayanara Berdan HayudiniNo ratings yet
- 10 - NYC 2021 COA Audit Report Part2 - Observations and RecommDocument66 pages10 - NYC 2021 COA Audit Report Part2 - Observations and RecommVERA FilesNo ratings yet
- Typical Signs and Symptoms of Psychiatric Illness DefinedDocument6 pagesTypical Signs and Symptoms of Psychiatric Illness DefinedElijah Manuel BibayNo ratings yet
- Mental Health Is Defined As "A State of Well-Being in Which Every IndividualDocument7 pagesMental Health Is Defined As "A State of Well-Being in Which Every IndividualmejulNo ratings yet
- Hildegard Peplaus Theory of Interpersonal RelationsDocument101 pagesHildegard Peplaus Theory of Interpersonal Relationsapi-384387326No ratings yet
- Bataan Case EditedDocument21 pagesBataan Case EditedCham Rafaela ConeseNo ratings yet
- The Mental Status ExamDocument7 pagesThe Mental Status ExamAnonymous ewPKlLWtfhNo ratings yet
- Concepts of Community CHN2 090120Document62 pagesConcepts of Community CHN2 090120Pucha MorinNo ratings yet
- Health Assessment #1Document15 pagesHealth Assessment #1Hazel Eñga Tiam WatNo ratings yet
- Case Presentation Second Year 2nd SemesterDocument36 pagesCase Presentation Second Year 2nd SemesterJohn Robert PescadorNo ratings yet
- Date/Hour of Shift Focus Note ProgressDocument2 pagesDate/Hour of Shift Focus Note Progressako at ang exoNo ratings yet
- Field Study 1: University of Caloocan CityDocument7 pagesField Study 1: University of Caloocan CityLovelyn MaristelaNo ratings yet
- National Program On Mental HealthDocument14 pagesNational Program On Mental HealthBee Anne Biñas100% (1)
- Informatics Solution For Emergency Preparedness and ResponseDocument4 pagesInformatics Solution For Emergency Preparedness and ResponseLuisseBeaI.BrazaNo ratings yet
- Sample 3Document42 pagesSample 3VeniceNo ratings yet
- OxygenationDocument12 pagesOxygenationCherry Lou Guanzing100% (1)
- Brokenshire College Socsksargen, Inc.: NCM 100-Theorerical Foundations in NursingDocument8 pagesBrokenshire College Socsksargen, Inc.: NCM 100-Theorerical Foundations in NursingKeren Happuch EspirituNo ratings yet
- Buergers Disease Concept MapDocument1 pageBuergers Disease Concept MapElmer Dizon100% (1)
- MilieuDocument17 pagesMilieuAntro BerrinNo ratings yet
- Department of Health - Leprosy Control Program - 2011-11-08Document9 pagesDepartment of Health - Leprosy Control Program - 2011-11-08daryl ann dep-asNo ratings yet
- Branded Vs Unbranded GenericsDocument2 pagesBranded Vs Unbranded GenericsYashaswiPathak100% (2)
- Department of HealthDocument22 pagesDepartment of HealthToyour EternityNo ratings yet
- Oxygen InhalationDocument26 pagesOxygen InhalationdaisyNo ratings yet
- Taking Charge of Nursing PracticeDocument59 pagesTaking Charge of Nursing PracticeMeia JaycelNo ratings yet
- Eight Elements of Primary Health Care (AlmaDocument4 pagesEight Elements of Primary Health Care (AlmaChristina GutierrezNo ratings yet
- Historical Background of Psychological Testing and AssessmentDocument4 pagesHistorical Background of Psychological Testing and AssessmentAndleeb AbbasNo ratings yet
- National Nutrition ProgrammeDocument37 pagesNational Nutrition ProgrammeEli Zza KoiralaNo ratings yet
- OxytocinDocument1 pageOxytocinjhinNo ratings yet
- FINAL Nursing ThesisDocument67 pagesFINAL Nursing ThesisAgronaSlaughter0% (1)
- Community Health Nursing 100 by JhunDocument22 pagesCommunity Health Nursing 100 by JhunJhun Echipare100% (5)
- Rle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingDocument6 pagesRle Module Rle Unit Week: Bachelor of Science in Nursing: Rle NCM 105 - Psychiatric NursingAllisson BeckersNo ratings yet
- TRESIBADocument16 pagesTRESIBARaina96No ratings yet
- Transcultural Perspective in Nursing Care For Children PDFDocument41 pagesTranscultural Perspective in Nursing Care For Children PDFJade CatubayNo ratings yet
- PhobiaDocument17 pagesPhobiaastha singhNo ratings yet
- Scizophrenia NCPDocument1 pageScizophrenia NCPKholid Abu Mohammad AlfaizinNo ratings yet
- Psychiatric Nursing 1Document17 pagesPsychiatric Nursing 1Marichu BajadoNo ratings yet
- A Cross-Sectional Survey of Knowledge, Attitude and Practice Associated With COVID-19 Among Undergraduate Students in ChinaDocument8 pagesA Cross-Sectional Survey of Knowledge, Attitude and Practice Associated With COVID-19 Among Undergraduate Students in Chinaandris mejia alvarezNo ratings yet
- Questionnaire Proforma - Vaccine Hesitancy (ENGLISH)Document5 pagesQuestionnaire Proforma - Vaccine Hesitancy (ENGLISH)krishna SarmaNo ratings yet
- 314 Lecture Module RevDocument92 pages314 Lecture Module RevMaica LectanaNo ratings yet
- Acceptance and Attitude Toward Covid-19 Vaccination: A Cross-Sectional Study From Udaipur DistrictDocument8 pagesAcceptance and Attitude Toward Covid-19 Vaccination: A Cross-Sectional Study From Udaipur DistrictIJAR JOURNALNo ratings yet
- EsophagealDiverticula StatPearls NCBIBookshelfDocument9 pagesEsophagealDiverticula StatPearls NCBIBookshelfInês PriorNo ratings yet
- Milieu TherapyDocument17 pagesMilieu TherapyMaine LamireNo ratings yet
- Proposing A Solution Teenage PregnancyDocument5 pagesProposing A Solution Teenage PregnancyJacques OwokelNo ratings yet
- Smiling Therapy Positive Effects On Mental HealthDocument6 pagesSmiling Therapy Positive Effects On Mental HealthSyazNo ratings yet
- EthicsDocument1 pageEthicsNadineNo ratings yet
- NCM 117J (Maladaptive Pattern of Behavior) : Overview of Psychiatric Mental Health Nursing Module 1/7Document41 pagesNCM 117J (Maladaptive Pattern of Behavior) : Overview of Psychiatric Mental Health Nursing Module 1/7Abdelmar Susulan100% (1)
- Types and Indications of CathetersDocument16 pagesTypes and Indications of CathetersMARYAM ASIMNo ratings yet
- Chapter IiDocument5 pagesChapter IiPeterson BanuaNo ratings yet
- Bipolar 1Document43 pagesBipolar 1rtishaiiNo ratings yet
- Mental Health ServicesDocument3 pagesMental Health ServicesAntonette NangNo ratings yet
- Response of The Office of The Court AdministratorDocument1 pageResponse of The Office of The Court AdministratorVERA FilesNo ratings yet
- DPWH DMC 81, S. 2023, With Memorandum Circular No. 39, S. 2023 From The Office of The PresidentDocument3 pagesDPWH DMC 81, S. 2023, With Memorandum Circular No. 39, S. 2023 From The Office of The PresidentVERA FilesNo ratings yet
- LTO Administrative Order No. AHS-2008-015Document5 pagesLTO Administrative Order No. AHS-2008-015VERA FilesNo ratings yet
- Participation Report: Col Braulio B Balbas JRDocument7 pagesParticipation Report: Col Braulio B Balbas JRVERA FilesNo ratings yet
- 11 - NYC 2020 COA Report Part3 - Status of PY's RecommDocument13 pages11 - NYC 2020 COA Report Part3 - Status of PY's RecommVERA FilesNo ratings yet
- 2022 Yearender - Types of Satire AttacksDocument3 pages2022 Yearender - Types of Satire AttacksVERA FilesNo ratings yet
- 2022 Yearender - Why Did Satire AppearDocument4 pages2022 Yearender - Why Did Satire AppearVERA FilesNo ratings yet
- Telegram On Marcos' Presscon - Feb. 24, 1986Document2 pagesTelegram On Marcos' Presscon - Feb. 24, 1986VERA FilesNo ratings yet
- 13 - NYC 2019 COA Report Part3 - Status of PY's RecommedationDocument8 pages13 - NYC 2019 COA Report Part3 - Status of PY's RecommedationVERA FilesNo ratings yet
- The Manila SunDocument1 pageThe Manila SunVERA FilesNo ratings yet
- 10 - NYC 2018 COA Report Part2 - Observations and RecommDocument19 pages10 - NYC 2018 COA Report Part2 - Observations and RecommVERA FilesNo ratings yet
- Memorandum For The President From The Governor of Ilocos Norte, 22 March 1984Document7 pagesMemorandum For The President From The Governor of Ilocos Norte, 22 March 1984VERA FilesNo ratings yet
- The Sandiganbayan Verdict SumDocument14 pagesThe Sandiganbayan Verdict SumVERA FilesNo ratings yet
- Adea To VerDocument1 pageAdea To VerVERA FilesNo ratings yet
- Supreme Court Public Information OfficeDocument1 pageSupreme Court Public Information OfficeVERA FilesNo ratings yet
- 11 - NYC 2019 COA Report Part2 - Observations and RecommDocument37 pages11 - NYC 2019 COA Report Part2 - Observations and RecommVERA FilesNo ratings yet
- Memorandum For The President From The Governor of Ilocos Norte, 11 June 1984Document2 pagesMemorandum For The President From The Governor of Ilocos Norte, 11 June 1984VERA FilesNo ratings yet
- Cendana's Information ProgramDocument5 pagesCendana's Information ProgramVERA FilesNo ratings yet
- 06-Ople Memo On Cavite PC CommanderDocument2 pages06-Ople Memo On Cavite PC CommanderVERA FilesNo ratings yet
- Implementing Rules and Regulations of RA 11346 and RA 11467Document8 pagesImplementing Rules and Regulations of RA 11346 and RA 11467VERA FilesNo ratings yet
- 2016 Memo Re Handling of Presidential FlightsDocument1 page2016 Memo Re Handling of Presidential FlightsVERA FilesNo ratings yet
- 03 Ople Campaign Plan Memo - P 16 To 34Document19 pages03 Ople Campaign Plan Memo - P 16 To 34VERA FilesNo ratings yet
- SEC Order Dated 28 June 2022 - in Re Rappler, Inc. and Rappler Holdings Corp.Document12 pagesSEC Order Dated 28 June 2022 - in Re Rappler, Inc. and Rappler Holdings Corp.VERA Files100% (1)
- 03 Ople Campaign Plan Memo - P 1 To 15Document15 pages03 Ople Campaign Plan Memo - P 1 To 15VERA FilesNo ratings yet
- 02-Memorandum and Attachments From Black, Manafort, Stone and Kelley (Proof of Marcos Regime Engagement)Document7 pages02-Memorandum and Attachments From Black, Manafort, Stone and Kelley (Proof of Marcos Regime Engagement)VERA FilesNo ratings yet
- Office of The Secretary: Media Questions, 08 March 2022 Questions: Responses: Carolyn Bonquin (CNN)Document7 pagesOffice of The Secretary: Media Questions, 08 March 2022 Questions: Responses: Carolyn Bonquin (CNN)VERA FilesNo ratings yet
- DOH, DepEd, DOF Call To Veto Vape BillDocument23 pagesDOH, DepEd, DOF Call To Veto Vape BillVERA FilesNo ratings yet
- Polypropylene Homo Polymer Injection Molding: Provisional Technical DatasheetDocument2 pagesPolypropylene Homo Polymer Injection Molding: Provisional Technical DatasheetMohit MohataNo ratings yet
- COLLEGE OF HEALTH SCIENCE Department of Anesthesia Research ProposalDocument29 pagesCOLLEGE OF HEALTH SCIENCE Department of Anesthesia Research Proposalmihret tedla100% (1)
- Beige and Blue Minimal Modern Thesis Defense PresentationDocument13 pagesBeige and Blue Minimal Modern Thesis Defense PresentationSaimon RumolNo ratings yet
- KS7710-13 - VERTICAL LIFELINE WEB - Manual-MinDocument13 pagesKS7710-13 - VERTICAL LIFELINE WEB - Manual-Mintyler CLausNo ratings yet
- (Doctor Who - New Series Adventures 63) Cole, Steve - Doctor Who - Combat MagicksDocument180 pages(Doctor Who - New Series Adventures 63) Cole, Steve - Doctor Who - Combat MagickssansNo ratings yet
- Commonly Confused WordsDocument3 pagesCommonly Confused WordsNhật MaiNo ratings yet
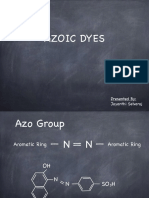
- Azoic Dyes: Presented By: Jayanthi SelvarajDocument13 pagesAzoic Dyes: Presented By: Jayanthi Selvarajdona biswasNo ratings yet
- Chapter 3Document3 pagesChapter 3Jom BonhayagNo ratings yet
- Presentation ON Rural BankDocument13 pagesPresentation ON Rural BankJiten AgrawalNo ratings yet
- Parties and Case No. Controversy or Issue Does NLRC Have Jurisdiction? Reason What Happened To The CaseDocument4 pagesParties and Case No. Controversy or Issue Does NLRC Have Jurisdiction? Reason What Happened To The CaseHiezll Wynn R. RiveraNo ratings yet
- 2nd Quarter Tle 10Document3 pages2nd Quarter Tle 10lovely joy dahuyaNo ratings yet
- Second Quarter TVE7 Pre TestDocument4 pagesSecond Quarter TVE7 Pre TestMary TraniNo ratings yet
- Neglect Affidavit - SampleDocument2 pagesNeglect Affidavit - SampleJona MayNo ratings yet
- Reproduction: The Diversity of Fish Reproduction: An IntroductionDocument3 pagesReproduction: The Diversity of Fish Reproduction: An IntroductioniqyuwidyaNo ratings yet
- Financial Accounting 1: Chapter 5 Cash and Short Term InvestmentDocument31 pagesFinancial Accounting 1: Chapter 5 Cash and Short Term InvestmentCabdiraxmaan GeeldoonNo ratings yet
- Battery Technical SpecificationsDocument16 pagesBattery Technical SpecificationsLeela Krishna VegiNo ratings yet
- Community Diagnosis 2Document225 pagesCommunity Diagnosis 2Justine MembridoNo ratings yet
- V20 2-Page Elder Ravnos InteractiveDocument2 pagesV20 2-Page Elder Ravnos InteractiveGogoNo ratings yet
- GMCB05B23124H1EU Amphenol Commercial ProductsDocument4 pagesGMCB05B23124H1EU Amphenol Commercial ProductsAmin JalaliNo ratings yet
- Cad DrawingDocument11 pagesCad DrawingGreen MyanmarNo ratings yet
- Hotpoint Ariston WML 601 Eu PDFDocument48 pagesHotpoint Ariston WML 601 Eu PDFDaliborka Burtić100% (1)
- CEE 41 Child Development and Care For Special Needs SEMESTER 1,2020 Assessment 2Document9 pagesCEE 41 Child Development and Care For Special Needs SEMESTER 1,2020 Assessment 2malisha chandNo ratings yet
- Thermal Stress Thermal Strains: Bibin ChidambaranathanDocument18 pagesThermal Stress Thermal Strains: Bibin ChidambaranathanDr. BIBIN CHIDAMBARANATHANNo ratings yet
- Ethinylestradiol As Betadex Calthrate 0.03mg + Drospirenone 3mg + Levomefolate Calcium 0.451mg (Yasmin Plus)Document23 pagesEthinylestradiol As Betadex Calthrate 0.03mg + Drospirenone 3mg + Levomefolate Calcium 0.451mg (Yasmin Plus)ddandan_2No ratings yet
- Adaptations Class6 Sci NDocument2 pagesAdaptations Class6 Sci NravilullaNo ratings yet