You might also like
- Advanced Practice and Leadership in Radiology NursingFrom EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossNo ratings yet
- Reaction ResearchDocument5 pagesReaction Researchapi-282416142No ratings yet
- Medication Errors - EditedDocument7 pagesMedication Errors - EditedHezron RonoNo ratings yet
- Nurses Compliance Towards Infection Control Practices at Sulu Sanitarium and General HospitalDocument12 pagesNurses Compliance Towards Infection Control Practices at Sulu Sanitarium and General HospitalJournal of Interdisciplinary PerspectivesNo ratings yet
- Reflection 1Document15 pagesReflection 1Reece JMNo ratings yet
- Reduce MedicationDocument12 pagesReduce MedicationDalia Talaat WehediNo ratings yet
- A Thesis (Proposal) Presented To The Faculty of The College of Nursing Adamson UniversityDocument22 pagesA Thesis (Proposal) Presented To The Faculty of The College of Nursing Adamson UniversityRaidis PangilinanNo ratings yet
- d1Document2 pagesd1charityachieng38No ratings yet
- NURS 682 Care Coordination and Role of The Advanced Practice NurseDocument3 pagesNURS 682 Care Coordination and Role of The Advanced Practice NurseParya VNo ratings yet
- Knowledge and Practice of Nursing Staff Towards InfectionDocument13 pagesKnowledge and Practice of Nursing Staff Towards InfectionZein AhmadNo ratings yet
- IdentidadDocument12 pagesIdentidadEdgarsito AyalaNo ratings yet
- NRS 2000Document13 pagesNRS 2000Hamza HaiderNo ratings yet
- Medication Errors 111765Document7 pagesMedication Errors 111765akko aliNo ratings yet
- Role of ResearchDocument5 pagesRole of ResearchAiman SiddiquiNo ratings yet
- Nurses' Adherence To Patient Safety Principles: A Systematic ReviewDocument15 pagesNurses' Adherence To Patient Safety Principles: A Systematic ReviewWidia Hertina PutriNo ratings yet
- 1 s2.0 S2049080121000595 Main1Document6 pages1 s2.0 S2049080121000595 Main1Devina ArrandhikasariNo ratings yet
- The Topic ofDocument3 pagesThe Topic ofaineyboneyNo ratings yet
- Epidemiology NursingDocument2 pagesEpidemiology NursingDhAiRyA ArOrA100% (2)
- Corresponding Author: Mojtaba Vaismoradi, Faculty of Professional Studies, Nord UniversityDocument24 pagesCorresponding Author: Mojtaba Vaismoradi, Faculty of Professional Studies, Nord UniversityTeddy Kurniady ThaherNo ratings yet
- Medication AssignmentDocument5 pagesMedication Assignmentapi-525323558No ratings yet
- 2018 - Khalil & LeeDocument12 pages2018 - Khalil & LeeazeemathmariyamNo ratings yet
- @EVIDENCE BASED PRACTICE - EditedDocument5 pages@EVIDENCE BASED PRACTICE - EditedSir Ben MwauNo ratings yet
- Infection Prevention by Nurses - EditedDocument6 pagesInfection Prevention by Nurses - EditedAllan DavisNo ratings yet
- Jayson NovellesDocument38 pagesJayson Novellesaronara dalampasiganNo ratings yet
- NURS-FPX 4010 Interdisciplinary Plan ProposalDocument8 pagesNURS-FPX 4010 Interdisciplinary Plan ProposalIrene WafulaNo ratings yet
- Ijarm: International Journal of Advanced Research in Management (Ijarm)Document11 pagesIjarm: International Journal of Advanced Research in Management (Ijarm)IAEME PublicationNo ratings yet
- Sample Research ProposalDocument43 pagesSample Research ProposalLuis LazaroNo ratings yet
- PSJ - Volume 8 - Issue 1 - Pages 13-23Document11 pagesPSJ - Volume 8 - Issue 1 - Pages 13-23mauliana mardhira fauzaNo ratings yet
- NURS4020 Ashley Assessment1 Attemp1Document6 pagesNURS4020 Ashley Assessment1 Attemp1ashleyNo ratings yet
- Hanif Lila Nursing EditedDocument7 pagesHanif Lila Nursing EditedHanif LilaNo ratings yet
- Diabetes Mellitus Autoimmune Insulin Beta Cells Pancreas Polyuria Polydipsia PolyphagiaDocument37 pagesDiabetes Mellitus Autoimmune Insulin Beta Cells Pancreas Polyuria Polydipsia PolyphagiaVishuNo ratings yet
- Knowledge, Attitude and Practice Towards Patient Safety Among Nurses Working at Selected Hospitals in Mogadishu-SomaliaDocument51 pagesKnowledge, Attitude and Practice Towards Patient Safety Among Nurses Working at Selected Hospitals in Mogadishu-Somaliasalman ibrahimNo ratings yet
- Research Nurse FinDocument5 pagesResearch Nurse FinFredrickNo ratings yet
- Effectiveness of Infection Control Standers On Practice Among Health Care Personnel Working in MCH Centers at Quena GovernorateDocument10 pagesEffectiveness of Infection Control Standers On Practice Among Health Care Personnel Working in MCH Centers at Quena GovernorateIOSRjournalNo ratings yet
- Patience Compliance - Edited.editedDocument4 pagesPatience Compliance - Edited.editedVincent JosephNo ratings yet
- Nurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesDocument5 pagesNurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesShiee Nevhie ParaDinata WapersNo ratings yet
- Critical Thinking Exercise - As A Change AgentDocument8 pagesCritical Thinking Exercise - As A Change AgentDennis Nabor Muñoz, RN,RMNo ratings yet
- Reflective JournalsDocument19 pagesReflective JournalsisisvlvtNo ratings yet
- The Use of Review of System AsDocument34 pagesThe Use of Review of System AsEva SahabNo ratings yet
- Artikel Bahasa Inggris Alda Depi ArieDocument7 pagesArtikel Bahasa Inggris Alda Depi ArieAlda DepiariNo ratings yet
- Literature Review ExampleDocument14 pagesLiterature Review ExampleZahra'a AlmeerNo ratings yet
- Research Helps Nurses Determine Effective Best Practices and Improve Patient CareDocument3 pagesResearch Helps Nurses Determine Effective Best Practices and Improve Patient CareAziil LiizaNo ratings yet
- Preventing Hospital Infections: Hygiene PracticesDocument10 pagesPreventing Hospital Infections: Hygiene PracticesSamwel KangyNo ratings yet
- FPX4020 WilsonChelsea Assessment4 1Document17 pagesFPX4020 WilsonChelsea Assessment4 1FrancisNo ratings yet
- Related LiteratureDocument7 pagesRelated LiteratureKrahNo ratings yet
- KNOWLEDGE AND ACTUAL PRACTICES ON INFECTIONCONTROL OF NURSING STUDENTS University of BoholDocument19 pagesKNOWLEDGE AND ACTUAL PRACTICES ON INFECTIONCONTROL OF NURSING STUDENTS University of BoholMark Johnuel DuavisNo ratings yet
- Hewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingDocument17 pagesHewison NURSES IDENTIFICATION AND REPORTING OF MEDICATION ERRORS Journal Clinical NursingCatrin_HutaurukNo ratings yet
- Thesis Prevention of Nosocomial Infections As Percieved by Staff NursesDocument7 pagesThesis Prevention of Nosocomial Infections As Percieved by Staff NursesDhonnalyn Amene Caballero100% (1)
- NursDocument31 pagesNursRaluca DumitrascuNo ratings yet
- Ethical Issues in Healthcare ManagementDocument44 pagesEthical Issues in Healthcare ManagementTravel with NiroNo ratings yet
- B 405Document14 pagesB 405NYONGKERNo ratings yet
- Effectiveness of Formal Observation in Inpatient Psychiatry in Preventing Adverse Outcomes: The State of The ScienceDocument7 pagesEffectiveness of Formal Observation in Inpatient Psychiatry in Preventing Adverse Outcomes: The State of The Sciencelovely99_dyahNo ratings yet
- APNs: Access, Cost, Quality Care & EnvironmentsDocument6 pagesAPNs: Access, Cost, Quality Care & EnvironmentsMellyne SallyNo ratings yet
- Law and Ethics Draft Grammatically CheckedDocument5 pagesLaw and Ethics Draft Grammatically CheckedAlvin Joseph PinedaNo ratings yet
- Chapter I PandaraDocument4 pagesChapter I Pandarasharief.aa90No ratings yet
- Caring Behavior and Associated Factors Among Nurses Working in Jimma University Specialized Hospital, Oromia, Southwest Ethiopia, 2019Document7 pagesCaring Behavior and Associated Factors Among Nurses Working in Jimma University Specialized Hospital, Oromia, Southwest Ethiopia, 2019Ryrey Abraham PacamanaNo ratings yet
- Collaborative Care Between Nurse Practitioners and Primary Care PhysiciansDocument11 pagesCollaborative Care Between Nurse Practitioners and Primary Care PhysiciansLeek AgoessNo ratings yet
- Improving Safety On High-Alert MedicationDocument48 pagesImproving Safety On High-Alert MedicationLenny SucalditoNo ratings yet
- Artikel 3 Berland 2017Document8 pagesArtikel 3 Berland 2017Eline DebaereNo ratings yet
- 420 Research PaperDocument12 pages420 Research Paperapi-372913673No ratings yet
- Running Head: Principles of Finance 1Document12 pagesRunning Head: Principles of Finance 1Best EssaysNo ratings yet
- Insert Surname 1: TH THDocument9 pagesInsert Surname 1: TH THBest EssaysNo ratings yet
- Running Head: Pharmacology and Diverse Populations: Bangladesh. 1Document7 pagesRunning Head: Pharmacology and Diverse Populations: Bangladesh. 1Best EssaysNo ratings yet
- ORDER 26693 BrochureDocument2 pagesORDER 26693 BrochureBest EssaysNo ratings yet
- Order 26693Document4 pagesOrder 26693Best EssaysNo ratings yet
- Literature ReviewDocument5 pagesLiterature ReviewBest EssaysNo ratings yet
- Running Head: HISTORY 1: American History Questions Name of Student Name of Institution DateDocument10 pagesRunning Head: HISTORY 1: American History Questions Name of Student Name of Institution DateBest EssaysNo ratings yet
- Running Head: HISTORY 1: American History Questions Name of Student Name of Institution DateDocument15 pagesRunning Head: HISTORY 1: American History Questions Name of Student Name of Institution DateBest EssaysNo ratings yet
- Running Head: Daily Life in The Middle East 1Document8 pagesRunning Head: Daily Life in The Middle East 1Best EssaysNo ratings yet
- Order 26705Document4 pagesOrder 26705Best EssaysNo ratings yet
- Critical Analysis of "Incognito: The Secret Lives of The Brain" by David EaglemanDocument9 pagesCritical Analysis of "Incognito: The Secret Lives of The Brain" by David EaglemanBest EssaysNo ratings yet
- Running Head: HISTORY 1: American History Questions Name of Student Name of Institution DateDocument14 pagesRunning Head: HISTORY 1: American History Questions Name of Student Name of Institution DateBest EssaysNo ratings yet
- Literature Review RevDocument4 pagesLiterature Review RevBest EssaysNo ratings yet
- Insert Surname 1: Family Court System Fails To Adopt The Fundamental Elements of A Fair TrialDocument13 pagesInsert Surname 1: Family Court System Fails To Adopt The Fundamental Elements of A Fair TrialBest EssaysNo ratings yet
- Running Head: ANTI-GLOBALIZATION 1Document10 pagesRunning Head: ANTI-GLOBALIZATION 1Best EssaysNo ratings yet
- Running Head: Gospel Teachings About The Holy Spirit 1Document7 pagesRunning Head: Gospel Teachings About The Holy Spirit 1Best EssaysNo ratings yet
- Running Head:: Quantitative Methods 1Document7 pagesRunning Head:: Quantitative Methods 1Best EssaysNo ratings yet
- Order 26653 RevDocument5 pagesOrder 26653 RevBest EssaysNo ratings yet
- Running Head: TEAMWORK 1: Teamwork Name of Student Name of Institution DateDocument8 pagesRunning Head: TEAMWORK 1: Teamwork Name of Student Name of Institution DateBest EssaysNo ratings yet
- Order 26634Document7 pagesOrder 26634Best EssaysNo ratings yet
- Name of Student Name of Professor Course Date: Insert Surname 1Document6 pagesName of Student Name of Professor Course Date: Insert Surname 1Best EssaysNo ratings yet
- Running Head: Case Study Seventy-ThreeDocument7 pagesRunning Head: Case Study Seventy-ThreeBest EssaysNo ratings yet
- Running Head: Healthcare Marketing Business Plan Project 1Document6 pagesRunning Head: Healthcare Marketing Business Plan Project 1Best EssaysNo ratings yet
- Preparedness For A Disaster 1: Running HeadDocument7 pagesPreparedness For A Disaster 1: Running HeadBest EssaysNo ratings yet
- Running Head: GENETIC DATA 1Document11 pagesRunning Head: GENETIC DATA 1Best EssaysNo ratings yet
- Running Head: Comparative Study of Asian American IdentityDocument8 pagesRunning Head: Comparative Study of Asian American IdentityBest EssaysNo ratings yet
- Running Head: Social Capital and Depression 1Document5 pagesRunning Head: Social Capital and Depression 1Best EssaysNo ratings yet
- Order 26639 RevDocument5 pagesOrder 26639 RevBest EssaysNo ratings yet
- Running Head: Case Study: Managing Information Technology Enterprise 1Document6 pagesRunning Head: Case Study: Managing Information Technology Enterprise 1Best EssaysNo ratings yet
- The Community As ClientDocument7 pagesThe Community As ClientDinia Esthu PangastutiNo ratings yet
- CHN TunayDocument38 pagesCHN Tunayjunathancortez123No ratings yet
- Breech Presentation - CGDocument13 pagesBreech Presentation - CGJun MingNo ratings yet
- DM No. 139 S. 2019Document18 pagesDM No. 139 S. 2019Jacqueline Hernandez MendozaNo ratings yet
- DewgardenDocument14 pagesDewgardenpushpa100% (4)
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsS M SarojNo ratings yet
- Understanding Disease Transmission DynamicsDocument14 pagesUnderstanding Disease Transmission Dynamicswulanda septianiNo ratings yet
- Community Health Nusing Exam EditedDocument9 pagesCommunity Health Nusing Exam EditedRosebel LaguraNo ratings yet
- Health CertificateDocument3 pagesHealth CertificateĐĂNG TRỊNH HẢINo ratings yet
- European Perinatal Health Report: Core Indicators of Health and Care for Pregnant Women and BabiesDocument180 pagesEuropean Perinatal Health Report: Core Indicators of Health and Care for Pregnant Women and BabiesTab101 WokingNo ratings yet
- KAP OF Personal Hygiene Among Students in Jazeera University Group A-1Document8 pagesKAP OF Personal Hygiene Among Students in Jazeera University Group A-1Maxamed DananNo ratings yet
- HIV PEP Checklist GuideDocument1 pageHIV PEP Checklist GuidededekfridayNo ratings yet
- A Disseration Submitted As A Partial Fulfilment For Award of The Diploma in Community Nutrition.Document8 pagesA Disseration Submitted As A Partial Fulfilment For Award of The Diploma in Community Nutrition.Prince HakimNo ratings yet
- Clinical Types of Epidemiological StudiesDocument3 pagesClinical Types of Epidemiological StudiesEduardo Proaño100% (1)
- Location Askec Office Toilet Id N/A For The Month of March-19 LegendDocument1 pageLocation Askec Office Toilet Id N/A For The Month of March-19 LegendBorislav VulićNo ratings yet
- Baby VaccineDocument3 pagesBaby VaccineNasrin SultanaNo ratings yet
- The Effects of Virus Variants On COVID-19 Vaccines: Inglés Nivel II Examen FinalDocument4 pagesThe Effects of Virus Variants On COVID-19 Vaccines: Inglés Nivel II Examen FinalDIEGONo ratings yet
- Breast Cancer in A Filipino Male - A Case Report (Rad Onco)Document6 pagesBreast Cancer in A Filipino Male - A Case Report (Rad Onco)Nico PlantadoNo ratings yet
- The SpirochetesDocument8 pagesThe SpirochetesAlthea Jam Grezshyl GaloNo ratings yet
- Family Nursing Care PlanDocument3 pagesFamily Nursing Care PlanColleen De la Rosa100% (1)
- 06 - Chapter 2 PDFDocument38 pages06 - Chapter 2 PDFSuraj DubeyNo ratings yet
- Kia NewDocument10 pagesKia NewFadhilah UlfahNo ratings yet
- Rguhs ThesisDocument4 pagesRguhs Thesissarahgriegoalbuquerque100% (2)
- Hubungan Pemberian Imunisasi Dasar Dengan Tumbuh Kembang Pada Bayi (0 - 1 Tahun) Di Puskesmaskembes Kecamatan Tombulu Kabupaten MinahasaDocument10 pagesHubungan Pemberian Imunisasi Dasar Dengan Tumbuh Kembang Pada Bayi (0 - 1 Tahun) Di Puskesmaskembes Kecamatan Tombulu Kabupaten MinahasatopanrkdNo ratings yet
- Philippines Health Information Systems in 40 CharactersDocument2 pagesPhilippines Health Information Systems in 40 CharactersCharles Mart Rabe-Rodriguez Hortilano100% (1)
- Vaccination or ImmunizationDocument4 pagesVaccination or ImmunizationPrincessNo ratings yet
- Students Health SurveyDocument1 pageStudents Health SurveyJulie Basbas-CruzNo ratings yet
- COVID 19 SOPs and Guidelines For Construction Sites PDFDocument8 pagesCOVID 19 SOPs and Guidelines For Construction Sites PDFshashanksaranNo ratings yet
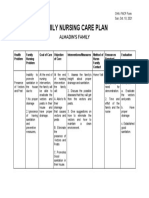
- FAMILY NURSING CARE PLAN - Almadin's FamilyDocument1 pageFAMILY NURSING CARE PLAN - Almadin's FamilyAngeline TaghapNo ratings yet
- Navigating Secondary Infertility With Homoeopathy: An Evidence-Based Case ReportDocument3 pagesNavigating Secondary Infertility With Homoeopathy: An Evidence-Based Case ReportDr Ananda Kumar PingaliNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Do You Believe in Magic?: The Sense and Nonsense of Alternative MedicineFrom EverandDo You Believe in Magic?: The Sense and Nonsense of Alternative MedicineNo ratings yet
- Epidemics and Society: From the Black Death to the PresentFrom EverandEpidemics and Society: From the Black Death to the PresentRating: 4.5 out of 5 stars4.5/5 (9)
- Uncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicFrom EverandUncontrolled Spread: Why COVID-19 Crushed Us and How We Can Defeat the Next PandemicNo ratings yet
- The Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsFrom EverandThe Wisdom of Plagues: Lessons from 25 Years of Covering PandemicsRating: 4.5 out of 5 stars4.5/5 (5)
- Epic Measures: One Doctor. Seven Billion Patients.From EverandEpic Measures: One Doctor. Seven Billion Patients.Rating: 4 out of 5 stars4/5 (13)
- The Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusFrom EverandThe Atlas of Disease: Mapping Deadly Epidemics and Contagion from the Plague to the CoronavirusRating: 4.5 out of 5 stars4.5/5 (10)
- The Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryFrom EverandThe Truth about Wuhan: How I Uncovered the Biggest Lie in HistoryRating: 4 out of 5 stars4/5 (6)
- Getting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsFrom EverandGetting Pregnant Naturally: Healthy Choices To Boost Your Chances Of Conceiving Without Fertility DrugsRating: 3.5 out of 5 stars3.5/5 (8)
- The HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedFrom EverandThe HPV Vaccine On Trial: Seeking Justice For A Generation BetrayedRating: 4.5 out of 5 stars4.5/5 (13)
- Nutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeFrom EverandNutritional and Therapeutic Interventions for Diabetes and Metabolic SyndromeNo ratings yet
- Deaths of Despair and the Future of CapitalismFrom EverandDeaths of Despair and the Future of CapitalismRating: 4.5 out of 5 stars4.5/5 (30)
- Fatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthFrom EverandFatal Conveniences: The Toxic Products and Harmful Habits That Are Making You Sick—and the Simple Changes That Will Save Your HealthRating: 4 out of 5 stars4/5 (7)
- Clean: Overcoming Addiction and Ending America’s Greatest TragedyFrom EverandClean: Overcoming Addiction and Ending America’s Greatest TragedyRating: 4 out of 5 stars4/5 (18)
- The Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanFrom EverandThe Bodies of Others: The New Authoritarians, COVID-19 and The War Against the HumanRating: 4.5 out of 5 stars4.5/5 (12)
- There Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceFrom EverandThere Are No Accidents: The Deadly Rise of Injury and Disaster—Who Profits and Who Pays the PriceRating: 4.5 out of 5 stars4.5/5 (15)
- The Transformation: Discovering Wholeness and Healing After TraumaFrom EverandThe Transformation: Discovering Wholeness and Healing After TraumaRating: 4 out of 5 stars4/5 (70)
- Arthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefFrom EverandArthritis Diet: Anti-inflammatory Diet for Arthritis Pain ReliefNo ratings yet
- War on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicFrom EverandWar on Ivermectin: The Medicine that Saved Millions and Could Have Ended the PandemicRating: 4 out of 5 stars4/5 (7)
- Doctored: The Disillusionment of an American PhysicianFrom EverandDoctored: The Disillusionment of an American PhysicianRating: 4 out of 5 stars4/5 (11)
- Microbiological Quality of FoodsFrom EverandMicrobiological Quality of FoodsL SlanetzNo ratings yet
- The Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthFrom EverandThe Gut-Immune Connection: How Understanding the Connection Between Food and Immunity Can Help Us Regain Our HealthNo ratings yet