You might also like
- VHigh Insulin RequirementDocument8 pagesVHigh Insulin RequirementSai NoonNo ratings yet
- Insulin Initiation and Titration in Patients T2DMDocument8 pagesInsulin Initiation and Titration in Patients T2DMkartikawensdiNo ratings yet
- Chun 2015 Atau ADA 2015Document8 pagesChun 2015 Atau ADA 2015hasan andrianNo ratings yet
- DiabetesDocument9 pagesDiabetesMsPocketbook HoarderNo ratings yet
- MnhwejcihdfjcnfekcnDocument8 pagesMnhwejcihdfjcnfekcnDr IslamNo ratings yet
- Practical Insulin: A Handbook for Prescribing ProvidersFrom EverandPractical Insulin: A Handbook for Prescribing ProvidersRating: 5 out of 5 stars5/5 (2)
- InsulinDocument2 pagesInsulinKristine YoungNo ratings yet
- Type III Hypersensitivity Reaction To Subcutaneous Insulin Preparations in A Type 1 DiabeticDocument5 pagesType III Hypersensitivity Reaction To Subcutaneous Insulin Preparations in A Type 1 DiabeticFeni Nurmia PutriNo ratings yet
- Case Study B.EDocument14 pagesCase Study B.EKOBE TOMAGANNo ratings yet
- Regular Insulin: A Drug Study OnDocument9 pagesRegular Insulin: A Drug Study OnSophia IbuyanNo ratings yet
- How Should We Manage Insulin Therapy Before SurgeryDocument3 pagesHow Should We Manage Insulin Therapy Before Surgerytsiko111No ratings yet
- Analogos de Insulina en DM 1 2017Document15 pagesAnalogos de Insulina en DM 1 2017LaurenArperNo ratings yet
- Module 9 ElaborateDocument6 pagesModule 9 ElaborateTrishaNo ratings yet
- Insulina Humana Menos Cara JAMADocument2 pagesInsulina Humana Menos Cara JAMApaulina farfanNo ratings yet
- Diabetes Medication 2017Document10 pagesDiabetes Medication 2017Nicolas Mauricio Rodriguez GonzalezNo ratings yet
- University of Northern PhilippinesDocument2 pagesUniversity of Northern PhilippinesDimple ComilangNo ratings yet
- Novolog (Insulin Aspart)Document3 pagesNovolog (Insulin Aspart)ENo ratings yet
- 327 Perioperative Insulin ManagementDocument6 pages327 Perioperative Insulin ManagementVinit KhemkaNo ratings yet
- Dok 21Document2 pagesDok 21dr. Noni PrisciliaNo ratings yet
- General Principles of Insulin Therapy in Diabetes Mellitus - UpToDateDocument25 pagesGeneral Principles of Insulin Therapy in Diabetes Mellitus - UpToDateNeider 1111No ratings yet
- Type 2 Diabetes Insulin Tactics GuideDocument30 pagesType 2 Diabetes Insulin Tactics GuideAlderkjNo ratings yet
- Monsalud - Drug StudyDocument5 pagesMonsalud - Drug StudyJanielle Christine MonsaludNo ratings yet
- Presentation TomorrowDocument8 pagesPresentation TomorrowRafik LakhdarNo ratings yet
- Cell Function in NewlyDocument6 pagesCell Function in NewlyJoseph PositivoNo ratings yet
- Universitatea "Ovidius" Din Constanta Facultatea de Farmacie Program de Studii FarmacieDocument12 pagesUniversitatea "Ovidius" Din Constanta Facultatea de Farmacie Program de Studii FarmacieAnamaria AvramNo ratings yet
- CHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaDocument6 pagesCHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaenesNo ratings yet
- Type 1 and 2 Diabetes Diagnosis, Symptoms, and TreatmentDocument5 pagesType 1 and 2 Diabetes Diagnosis, Symptoms, and TreatmentBrandon LewisNo ratings yet
- Diabetes MELLITUSDocument15 pagesDiabetes MELLITUSAshtua MandixNo ratings yet
- DRUG STUDY Insulin Humulin RDocument2 pagesDRUG STUDY Insulin Humulin RFrancesca Icalina Buensuceso100% (12)
- New Technologies and Therapies in The Management of DiabetesDocument8 pagesNew Technologies and Therapies in The Management of DiabetesArhaMozaNo ratings yet
- Diabetes SobrebasalizaciónDocument7 pagesDiabetes SobrebasalizaciónComisión Académica FCM - UNAHNo ratings yet
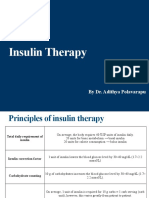
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Novolin R SQ (Regular Insulin)Document3 pagesNovolin R SQ (Regular Insulin)ENo ratings yet
- Lantus (Insulin Glargine)Document3 pagesLantus (Insulin Glargine)ENo ratings yet
- Laliberte 2010Document11 pagesLaliberte 2010iacob ancutaNo ratings yet
- Antidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 MayDocument54 pagesAntidiabetic Drugs. 12 May Modified 2016 of 2015 - 2017 11 17 Mayblue sapphireNo ratings yet
- Effective Use of Insulin Therapy in Type 2 DiabetesDocument7 pagesEffective Use of Insulin Therapy in Type 2 DiabetesmariohuangNo ratings yet
- REFERENCE: Brunner and Suddarth's Textbook of Medical-Surgical Nursing, 10th Edition, Volume 1, Page 1026Document3 pagesREFERENCE: Brunner and Suddarth's Textbook of Medical-Surgical Nursing, 10th Edition, Volume 1, Page 1026Charissa Magistrado De LeonNo ratings yet
- Antidiabetic Agents GuideDocument19 pagesAntidiabetic Agents GuideJames SoeNo ratings yet
- Insulin AdministrationDocument9 pagesInsulin AdministrationMonika JosephNo ratings yet
- 1 Case Report InsulinDocument4 pages1 Case Report InsulinNadine ShabrinaNo ratings yet
- Assessing Insulin Sensitivity Invivo 2007Document12 pagesAssessing Insulin Sensitivity Invivo 2007Afzal M NaeemNo ratings yet
- Gestational Diabetes Mellitus DefinitionDocument4 pagesGestational Diabetes Mellitus DefinitionTempoNo ratings yet
- Manejo de La DMGDocument5 pagesManejo de La DMGsandymejiaNo ratings yet
- Standards of Medical Care in Diabetesd2019: 9. Pharmacologic Approaches To Glycemic TreatmentDocument13 pagesStandards of Medical Care in Diabetesd2019: 9. Pharmacologic Approaches To Glycemic TreatmentRene Alexis Rodriguez JoaquinNo ratings yet
- Reversal of Type 1 Diabetes Using Plant-Based Diet: A Case StudyDocument3 pagesReversal of Type 1 Diabetes Using Plant-Based Diet: A Case StudyMananNo ratings yet
- VALDEZ - Nursing Process of Diabetes Mellitus PDFDocument4 pagesVALDEZ - Nursing Process of Diabetes Mellitus PDFDexel Lorren ValdezNo ratings yet
- Journal of Drug Delivery and Therapeutics: Current Challenges in Non-Invasive Insulin Drug Delivery System: A ReviewDocument7 pagesJournal of Drug Delivery and Therapeutics: Current Challenges in Non-Invasive Insulin Drug Delivery System: A ReviewkshitijNo ratings yet
- Insulin Therapy: A Personal Approach: Mayer B. DavidsonDocument13 pagesInsulin Therapy: A Personal Approach: Mayer B. DavidsonRetri AtikaNo ratings yet
- Insulin Autoimmune Syndrome Induced by Exogenous Insulin Injection: A Four-Case SeriesDocument6 pagesInsulin Autoimmune Syndrome Induced by Exogenous Insulin Injection: A Four-Case SeriesFeni Nurmia PutriNo ratings yet
- University of Luzon Nursing Care PlanDocument4 pagesUniversity of Luzon Nursing Care PlanMica KoreeneNo ratings yet
- Insulin and Antidiabetic Drugs: Prof - DR Asya RehmanDocument23 pagesInsulin and Antidiabetic Drugs: Prof - DR Asya RehmanGareth BaleNo ratings yet
- Case Report: Komal Tariq, MD Saira Tariq, MBBS Amanda M. Denney Queen, MDDocument5 pagesCase Report: Komal Tariq, MD Saira Tariq, MBBS Amanda M. Denney Queen, MDDekdesNo ratings yet
- Antidiabetic AgentDocument5 pagesAntidiabetic AgentChamique Gelle Kerlin C LingayoNo ratings yet
- Insulin Pharmacology Therapeutic Regimen and Priciple of Intensive Insulin Theraphy 2Document41 pagesInsulin Pharmacology Therapeutic Regimen and Priciple of Intensive Insulin Theraphy 2Dinar Danan SukmawatiNo ratings yet
- Acarbose Drug Study OverviewDocument3 pagesAcarbose Drug Study OverviewKian HerreraNo ratings yet
- ROLE OF STEROIDS IN REFRACTORY HYPOGLYCEMIA DUE TO AN OVERDOSE OF INSULIN GLARGINEDocument5 pagesROLE OF STEROIDS IN REFRACTORY HYPOGLYCEMIA DUE TO AN OVERDOSE OF INSULIN GLARGINEkcstincasNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Weeks 1-2 Carb Cycling Blueprint FINAL r1Document24 pagesWeeks 1-2 Carb Cycling Blueprint FINAL r1Umashanker VishwakarmaNo ratings yet
- Gaucher Disease Text A: Reading Test 12Document20 pagesGaucher Disease Text A: Reading Test 12Prsh Sanna Paudl0% (1)
- Visceral FatDocument5 pagesVisceral FatClint BodungenNo ratings yet
- Jais e Bruning (2017) Hypothalamic Inflammation in Obesity and Metabolic DiseaseDocument10 pagesJais e Bruning (2017) Hypothalamic Inflammation in Obesity and Metabolic DiseaseAna Flávia SordiNo ratings yet
- Mobilizzazione LipidicaDocument21 pagesMobilizzazione LipidicaLuca PellaNo ratings yet
- Drugs For Diabetes (Part 1)Document6 pagesDrugs For Diabetes (Part 1)حوراء عارف الموسويNo ratings yet
- Onnit DietDocument55 pagesOnnit DietGurram SrihariNo ratings yet
- ADA Type 2 Diabetes in ChildrensDocument10 pagesADA Type 2 Diabetes in ChildrensCho Maharani Rijhigo BaeNo ratings yet
- GDM (Gestational Diabetes Mellitus) PresentationDocument32 pagesGDM (Gestational Diabetes Mellitus) PresentationMovies 4 YouNo ratings yet
- Scientific Evidence of Diets For Weight Loss Different Macronutrient... (BITAN ČLANAK)Document11 pagesScientific Evidence of Diets For Weight Loss Different Macronutrient... (BITAN ČLANAK)mirkoNo ratings yet
- Aboite and About - February 2012Document32 pagesAboite and About - February 2012KPC Media Group, Inc.No ratings yet
- Family Medicine Shelf ReviewDocument69 pagesFamily Medicine Shelf ReviewnomansnNo ratings yet
- My ThesisDocument198 pagesMy Thesisshaimaa599100% (1)
- A Crash Course in Insulin Resistance PDFDocument12 pagesA Crash Course in Insulin Resistance PDFRajesh100% (1)
- Insulin ResistanceDocument48 pagesInsulin ResistanceLavina JainNo ratings yet
- Metabolic Syndrome: Causes and Risks of Cluster of 5 ConditionsDocument119 pagesMetabolic Syndrome: Causes and Risks of Cluster of 5 ConditionsMudassar SattarNo ratings yet
- Diabetes Mellitus FP NotebookDocument11 pagesDiabetes Mellitus FP NotebookDibyendunarayan BidNo ratings yet
- Time Allowed: 3 Hours Maximum Marks: 100Document14 pagesTime Allowed: 3 Hours Maximum Marks: 100vandana61No ratings yet
- MNT Case Study 2Document4 pagesMNT Case Study 2api-344809505100% (2)
- Bill Sardi: The Vitamin Supplement Answer ManDocument7 pagesBill Sardi: The Vitamin Supplement Answer Mandinesh bhatiaNo ratings yet
- The Effects of Fat and Protein on Glycemic ResponsesDocument6 pagesThe Effects of Fat and Protein on Glycemic ResponsesRavi kumarNo ratings yet
- Rrarf!: by Matt StoneDocument62 pagesRrarf!: by Matt Stonepat557No ratings yet
- Healthy KetosysIntermittent FastingDocument64 pagesHealthy KetosysIntermittent Fastingrrajen195% (19)
- Insulin and Insulin ResistanceDocument21 pagesInsulin and Insulin ResistanceFisiologiaUFCG100% (1)
- 02.2012 ADA LB Abstracts - CovDocument55 pages02.2012 ADA LB Abstracts - CovEndang SetiawatiNo ratings yet
- Coronary Artery AtherosclerosisDocument25 pagesCoronary Artery AtherosclerosisShahrizal Che JamelNo ratings yet
- Taiwanese Journal of Obstetrics & Gynecology: Ching-Ju Shen, Shih-Han Wang, Chien-Hung Lee, Te-Fu ChanDocument4 pagesTaiwanese Journal of Obstetrics & Gynecology: Ching-Ju Shen, Shih-Han Wang, Chien-Hung Lee, Te-Fu ChanIman Ru-ancaNo ratings yet
- Diabetes Global STI Kim EnricoDocument5 pagesDiabetes Global STI Kim EnricoKim Enrico JumarangNo ratings yet
- Roru Exoendo - PancreasDocument13 pagesRoru Exoendo - PancreasRitz CelsoNo ratings yet
- Diabetes Mellitus: Type 1 DM Type 2 DM Gestational DM Other TypesDocument20 pagesDiabetes Mellitus: Type 1 DM Type 2 DM Gestational DM Other Typesmohamed mowafeyNo ratings yet