You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Foundations of Operative Surgery An Introduction To Surgical TechniquesDocument165 pagesFoundations of Operative Surgery An Introduction To Surgical TechniquesTeodora-Valeria TolanNo ratings yet
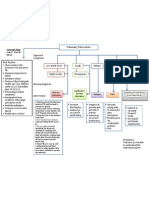
- Concept Map PTBDocument1 pageConcept Map PTBJoan Abardo100% (2)
- Che 225 Control of Communicable DiseasesDocument19 pagesChe 225 Control of Communicable DiseasesAbdullahi Bashir SalisuNo ratings yet
- MALNUTRITIONDocument42 pagesMALNUTRITIONWilliam C ChishaNo ratings yet
- The CestodesDocument16 pagesThe CestodesWilliam C ChishaNo ratings yet
- Complementary FeedingDocument53 pagesComplementary FeedingWilliam C ChishaNo ratings yet
- The Urinary System: Mr. M'hango GDocument50 pagesThe Urinary System: Mr. M'hango GWilliam C ChishaNo ratings yet
- The Trematodes (Flukes) Presented by Happy SimozuDocument93 pagesThe Trematodes (Flukes) Presented by Happy SimozuWilliam C ChishaNo ratings yet
- Failure of Immune SystemDocument21 pagesFailure of Immune SystemWilliam C Chisha100% (1)
- Complement System EdenDocument52 pagesComplement System EdenWilliam C ChishaNo ratings yet
- Analgesics: Non-Steroidal Anti-Inflammatory Drugs andDocument8 pagesAnalgesics: Non-Steroidal Anti-Inflammatory Drugs andWilliam C ChishaNo ratings yet
- Acquired ImmunityDocument22 pagesAcquired ImmunityWilliam C ChishaNo ratings yet
- Principles of Anatomy and Physiology: 14 EditionDocument62 pagesPrinciples of Anatomy and Physiology: 14 EditionWilliam C Chisha100% (1)
- Chapter III. GoutDocument28 pagesChapter III. GoutWilliam C ChishaNo ratings yet
- Chapter II. OsteoarthritisDocument23 pagesChapter II. OsteoarthritisWilliam C ChishaNo ratings yet
- Chapter Iv. Lumbago-Sciatica PDFDocument25 pagesChapter Iv. Lumbago-Sciatica PDFWilliam C ChishaNo ratings yet
- Tercera SemanaDocument9 pagesTercera SemanaJesús Torres MayaNo ratings yet
- Rachel Bray - ResumeDocument2 pagesRachel Bray - Resumeapi-625221885No ratings yet
- UntitledDocument17 pagesUntitledInggrid Aprilia ChristyNo ratings yet
- A Silent KillerDocument3 pagesA Silent KillerLinhNguyeNo ratings yet
- Icp Member Handbook Il PDFDocument36 pagesIcp Member Handbook Il PDFjohnNo ratings yet
- Physical Abuse Teaching SlidesDocument19 pagesPhysical Abuse Teaching SlidesbentoeNo ratings yet
- Columbia Asia Referral HospitalDocument9 pagesColumbia Asia Referral HospitalNeerajNo ratings yet
- Shellfish AllergyDocument23 pagesShellfish AllergyThessa Vee Capuno RioNo ratings yet
- Ncbi List of Books and Dental ArticlesDocument6 pagesNcbi List of Books and Dental ArticlesIulia Isacov0% (1)
- Modifiers-Table 122015 2Document25 pagesModifiers-Table 122015 2khatNo ratings yet
- Reflection Paper Pediatric Community-Acquired Pneumonia in The United StatesDocument2 pagesReflection Paper Pediatric Community-Acquired Pneumonia in The United StatesLecery Sophia WongNo ratings yet
- 11 Human Body SystemDocument3 pages11 Human Body SystemCris EnriquezNo ratings yet
- Family Laboratory For Medical Analysis: Test & SpecimenDocument1 pageFamily Laboratory For Medical Analysis: Test & SpecimenMohamad BadranNo ratings yet
- Acute Parenchymal Liver DiseaseDocument29 pagesAcute Parenchymal Liver Diseasejeevan ghimireNo ratings yet
- Imle 18.02.2013Document47 pagesImle 18.02.2013Nas Man100% (1)
- Semi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniDocument7 pagesSemi-Rigid Ureteroscopy: Indications, Tips, and Tricks: Lily A. Whitehurst Bhaskar K. SomaniUmar FarooqNo ratings yet
- The Conceptual Evolution of DSM 5Document391 pagesThe Conceptual Evolution of DSM 5monkey85222100% (3)
- Itpc PT ProcessDocument2 pagesItpc PT ProcessKyle MañiboNo ratings yet
- Treatment Modalities Applicable To The Psychiatric ClientDocument53 pagesTreatment Modalities Applicable To The Psychiatric Clientnickybore100% (1)
- National NORCET Test-9Document106 pagesNational NORCET Test-9SHIVANIINo ratings yet
- The Administration of Medications I. Speaking 'Administering Medications'Document5 pagesThe Administration of Medications I. Speaking 'Administering Medications'Meri AndaniNo ratings yet
- Diabetes Jigsaw ActivitiesDocument11 pagesDiabetes Jigsaw ActivitiesJacqueline CullieNo ratings yet
- Counseling TechniquesDocument60 pagesCounseling Techniquesdinalen0% (1)
- HIV Drug Chart (2021)Document1 pageHIV Drug Chart (2021)savNo ratings yet
- Bilateral OsteoarthritisDocument58 pagesBilateral OsteoarthritisMaya VilNo ratings yet
- Kleptomania Term PaperDocument6 pagesKleptomania Term Paperbctfnerif100% (1)
- Acid Fast StainDocument3 pagesAcid Fast StainMartina MicicNo ratings yet