You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5807)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- INBDEBooster Periodontics NotesDocument28 pagesINBDEBooster Periodontics NotesShawqi A100% (1)
- A New Method To Eliminate The Risk of Maxillary Sinusitis With Zygomatic ImplantsDocument9 pagesA New Method To Eliminate The Risk of Maxillary Sinusitis With Zygomatic ImplantsCaioSelaimenNo ratings yet
- Program Outline With LinksDocument4 pagesProgram Outline With Linksapi-240251657No ratings yet
- Cultural and Spiritual Diversity in NursingDocument63 pagesCultural and Spiritual Diversity in NursingKrisna May Buhisan Pecore100% (2)
- Tube Feeding in ChildrenDocument14 pagesTube Feeding in ChildrenClarestaNo ratings yet
- Intrapartum Assessment: Factors That Affect Oxygenation During LaborDocument10 pagesIntrapartum Assessment: Factors That Affect Oxygenation During LabornicewanNo ratings yet
- JSSWH - Volume 52 - Issue 2 - Pages 305-346Document42 pagesJSSWH - Volume 52 - Issue 2 - Pages 305-346jordan jubaNo ratings yet
- Stapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesDocument10 pagesStapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesLuis De jesus SolanoNo ratings yet
- Ann Rev Balic Et Al FinalDocument14 pagesAnn Rev Balic Et Al FinalFreddy A. ManayayNo ratings yet
- Nutrition Monitoring & Evaluation 2021Document32 pagesNutrition Monitoring & Evaluation 2021Dina Ade Wulan NuaritaNo ratings yet
- Community FNCPDocument7 pagesCommunity FNCPCarl Jefferson Pagulayan100% (1)
- National Guidelines For The Management of Tuberculosis in Children - 2Document77 pagesNational Guidelines For The Management of Tuberculosis in Children - 2Christy AmandaNo ratings yet
- CAstV Biochek Slacum WVPA 2017 PDFDocument23 pagesCAstV Biochek Slacum WVPA 2017 PDFJimeno Franscisco de los pozosNo ratings yet
- Diabetes ManualDocument242 pagesDiabetes Manualkapsicumad100% (1)
- Nephrotic SyndromeDocument84 pagesNephrotic SyndromeRahul DhakerNo ratings yet
- Guidelines For Evaluation and Assessment of Mental Illness and Procedure For CertificationDocument20 pagesGuidelines For Evaluation and Assessment of Mental Illness and Procedure For CertificationRasika Avinash GodboleNo ratings yet
- Direct Versus Indirect Inlayonlay Composite Restorations in Posterior Teeth. A Systematic Review and Meta-Analysis PDFDocument10 pagesDirect Versus Indirect Inlayonlay Composite Restorations in Posterior Teeth. A Systematic Review and Meta-Analysis PDFMel LlerenaNo ratings yet
- SentinaDocument10 pagesSentinaakayaNo ratings yet
- Jessica Parkus and Madison East Medically Compromised PatientDocument3 pagesJessica Parkus and Madison East Medically Compromised Patientapi-447657554No ratings yet
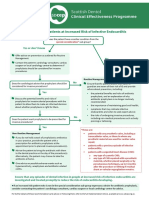
- SDCEP Antibiotic Prophylaxis Summary FlowchartDocument1 pageSDCEP Antibiotic Prophylaxis Summary FlowchartMahmoud EladawyNo ratings yet
- Service Master TemplateDocument14 pagesService Master TemplateRayrc Pvt LtdNo ratings yet
- Picopaper FinalDocument10 pagesPicopaper Finalapi-238698438No ratings yet
- 2 Infectious Disease EpidemiologyDocument62 pages2 Infectious Disease Epidemiologykindness jawoNo ratings yet
- Icd10 Congestive Heart FailureDocument2 pagesIcd10 Congestive Heart FailurerizkaNo ratings yet
- Introduction ThesisDocument36 pagesIntroduction Thesissourabh jakharNo ratings yet
- K1 - Initial AssessmentDocument34 pagesK1 - Initial Assessmentpuja argaNo ratings yet
- Health Care Delivery SystemDocument41 pagesHealth Care Delivery Systemankita100% (6)
- Cover LetterDocument2 pagesCover Letterapi-219168035No ratings yet
- Handouts - PeriopDocument79 pagesHandouts - PerioplibalibzyrelleNo ratings yet
- Monev Program Imunisasi Puskesmas Citapen Bulan Januari 2019Document5 pagesMonev Program Imunisasi Puskesmas Citapen Bulan Januari 2019Khoirunnisa DamayantiNo ratings yet