You might also like
- NI Chapter2Document2 pagesNI Chapter2Nthnl Czr88% (8)
- Aon Care GHS Claim FormDocument5 pagesAon Care GHS Claim FormGelson Herrera0% (5)
- Sail Ipd FormDocument2 pagesSail Ipd Formshami78% (9)
- Documentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsFrom EverandDocumentation for Skilled Nursing & Long-Term Care: A Guide for Occupational TherapistsNo ratings yet
- Horton CH 3 Test AnswersDocument4 pagesHorton CH 3 Test Answersscribddommini88% (8)
- Angel of Death - The Donald Harvey StoryDocument10 pagesAngel of Death - The Donald Harvey StoryMaria AthanasiadouNo ratings yet
- Family FLoater FormDocument6 pagesFamily FLoater FormSantosh KodereNo ratings yet
- PP CformDocument4 pagesPP CformHihiNo ratings yet
- BSIB GHS Claim FormDocument3 pagesBSIB GHS Claim FormmuhsinmohammedNo ratings yet
- Mediclaim 2012 Proposal FormDocument6 pagesMediclaim 2012 Proposal FormgaurnityanandaNo ratings yet
- Pre-Existing Conditions Disclosure Form: Page 1 of 2Document2 pagesPre-Existing Conditions Disclosure Form: Page 1 of 2celeenNo ratings yet
- Medical Application FormDocument3 pagesMedical Application FormBogdan Brdar100% (1)
- Attending Physicians Statement Crisis Cover Major Organ Transplant - 041222Document2 pagesAttending Physicians Statement Crisis Cover Major Organ Transplant - 041222max leeNo ratings yet
- Medical Application Form PDFDocument3 pagesMedical Application Form PDFHumanNo ratings yet
- Mumbai Claim FormDocument5 pagesMumbai Claim FormsunsangraNo ratings yet
- Attending Physicians Statement Crisis Cover Renal Failure - 041222Document2 pagesAttending Physicians Statement Crisis Cover Renal Failure - 041222max leeNo ratings yet
- Musculoskeletal Questionnaire Applicant 2020Document2 pagesMusculoskeletal Questionnaire Applicant 2020Kylle SaligumbaNo ratings yet
- All Medicare C73ac3dea5Document12 pagesAll Medicare C73ac3dea5shivamvijaymishra1703No ratings yet
- All Medicare C73ac3dea5Document12 pagesAll Medicare C73ac3dea5Pradeep SahuNo ratings yet
- Ahmedabad Claim FormDocument5 pagesAhmedabad Claim FormFirdaus PanthakyNo ratings yet
- Proposal Form New India Floater Mediclaim Policy 21012020 - 1Document6 pagesProposal Form New India Floater Mediclaim Policy 21012020 - 1aj iseNo ratings yet
- Medical Claim - Doctor'S Statement: Patient's Personal DetailsDocument3 pagesMedical Claim - Doctor'S Statement: Patient's Personal DetailsWeng Meng VISTANo ratings yet
- Igi - Ipd Claim FormDocument1 pageIgi - Ipd Claim FormMoaaz Khan100% (1)
- Hospitalization Reimbursment Claim FormDocument4 pagesHospitalization Reimbursment Claim FormFarhan aliNo ratings yet
- Proposal Form Ashakiran PDFDocument6 pagesProposal Form Ashakiran PDFSreejith Rajendran PillaiNo ratings yet
- Medical Application Form (New) - V3-2021!10!12 - RAKDocument3 pagesMedical Application Form (New) - V3-2021!10!12 - RAKAnkita NiravNo ratings yet
- Proposal Form New India Mediclaim Policy 01102021Document6 pagesProposal Form New India Mediclaim Policy 01102021abcdefabcNo ratings yet
- MAF - MednetDocument3 pagesMAF - MednetMuhammad Siddiuqi100% (1)
- Orient - Family Care - HAAD - Medical Application Form - Apr 2019Document7 pagesOrient - Family Care - HAAD - Medical Application Form - Apr 2019AAMIRNo ratings yet
- New Axa FormDocument2 pagesNew Axa FormAzrul Azuar Azrul Azuar100% (1)
- REV - Outpatient Claim Form - AIADocument2 pagesREV - Outpatient Claim Form - AIAYen SylvaniNo ratings yet
- AXA Hypertension QuestionnaireDocument2 pagesAXA Hypertension QuestionnaireClaudine Limasa TabudlongNo ratings yet
- OVHC Claim Form 102017 PDFDocument3 pagesOVHC Claim Form 102017 PDFtarmudiNo ratings yet
- Proposal Form New India Floater Mediclaim Policy-1Document7 pagesProposal Form New India Floater Mediclaim Policy-1Hemraj SonarNo ratings yet
- REV - Inpatient Claim Form - AIADocument2 pagesREV - Inpatient Claim Form - AIAYen SylvaniNo ratings yet
- Group and Individual Medical Claims FormDocument3 pagesGroup and Individual Medical Claims FormSheikh Alif Amzar BuxNo ratings yet
- Aon - Aia Ghs Claim Form - Oct 2014Document3 pagesAon - Aia Ghs Claim Form - Oct 2014John SmithNo ratings yet
- Maid Claim FormDocument4 pagesMaid Claim FormHihiNo ratings yet
- Medical Application Form: Insured Name: Inception DateDocument3 pagesMedical Application Form: Insured Name: Inception DateDidier G PeñuelaNo ratings yet
- Health Premium PlatinumDocument3 pagesHealth Premium Platinumகமலேஷ் குமார்No ratings yet
- Preauthorization Request Form - FinalDocument3 pagesPreauthorization Request Form - FinalRiya GhayelNo ratings yet
- Attending Physicians Statement Crisis Cover Muscular Dystrophy - 041222Document2 pagesAttending Physicians Statement Crisis Cover Muscular Dystrophy - 041222laraNo ratings yet
- Rev 3 RAWAT JALAN INDIVIDUAL InggrisDocument2 pagesRev 3 RAWAT JALAN INDIVIDUAL InggrisمولديياNo ratings yet
- FB Pregnancy-ComplicationDocument19 pagesFB Pregnancy-ComplicationHihiNo ratings yet
- NEW Takaful Hospital and Surgical Claim Form - Sun Life Malaysia Takaful PDFDocument4 pagesNEW Takaful Hospital and Surgical Claim Form - Sun Life Malaysia Takaful PDFamadkacakNo ratings yet
- Department of State Academic Exchanges Participant Medical History and Examination FormDocument8 pagesDepartment of State Academic Exchanges Participant Medical History and Examination FormNurman HidayatNo ratings yet
- Confidential Medical Certificate (Total and Permanent Disability) PDFDocument3 pagesConfidential Medical Certificate (Total and Permanent Disability) PDFJP PalamNo ratings yet
- Proposal Form New India Mediclaim PolicyDocument6 pagesProposal Form New India Mediclaim PolicyPavan Kumar NarbolikarNo ratings yet
- MET - Medical Claim Reimbursement Form in Patient - KWTDocument2 pagesMET - Medical Claim Reimbursement Form in Patient - KWTangeloriondo1217No ratings yet
- 2020 Medefend Notification Form Anne GeorginaDocument4 pages2020 Medefend Notification Form Anne GeorginaKevin Bartholomew LawsonNo ratings yet
- Arabian Scandinavian Insurance Co. PLC - Takaful: Medical Questionnaire FormDocument3 pagesArabian Scandinavian Insurance Co. PLC - Takaful: Medical Questionnaire FormAlbert BhattiNo ratings yet
- Insurnace Individual & Family FormDocument6 pagesInsurnace Individual & Family FormMuhammad SiddiuqiNo ratings yet
- NTUC Pa Paid Claim Form (08 2017)Document5 pagesNTUC Pa Paid Claim Form (08 2017)pat5355No ratings yet
- ME In-G Ie: Claim FormDocument4 pagesME In-G Ie: Claim FormnithiananthiNo ratings yet
- FB ClaimDocument14 pagesFB ClaimHihiNo ratings yet
- 1107398b-09a0 - Salaam Health Claim FormDocument2 pages1107398b-09a0 - Salaam Health Claim FormFarhan Ali100% (1)
- Covid-19 Test Claim FormDocument2 pagesCovid-19 Test Claim Formmuhammad anasNo ratings yet
- Fulbright Certificate of HealthDocument8 pagesFulbright Certificate of HealthLinda Klimavicius100% (1)
- PP MreportDocument5 pagesPP MreportHihiNo ratings yet
- Medical Insurance Hospitalisation Surgical Claim FormDocument2 pagesMedical Insurance Hospitalisation Surgical Claim FormAustin KeungNo ratings yet
- Medical Certificate of FitnessDocument2 pagesMedical Certificate of FitnessPraveen Kumar Madupu100% (1)
- Fitness To Practise FormDocument2 pagesFitness To Practise FormKazi Mobaidul Islam ShovonNo ratings yet
- A Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsFrom EverandA Guide for Medical Case Managers: Stop Loss Insurance for Medical ProfessionalsNo ratings yet
- TaliDocument1 pageTaliKalyesubula Mahad AraaliNo ratings yet
- EAC Anthem in Kiswahili: Verse 1Document1 pageEAC Anthem in Kiswahili: Verse 1Ezra Tumusiime77% (13)
- 06.03.2020 - 12.03.2020 SuccessfulDocument9 pages06.03.2020 - 12.03.2020 SuccessfulKalyesubula Mahad AraaliNo ratings yet
- Policy Statement As at 03-Mar-2020: Print Date: Tuesday, March 3, 2020Document1 pagePolicy Statement As at 03-Mar-2020: Print Date: Tuesday, March 3, 2020Kalyesubula Mahad AraaliNo ratings yet
- Policy Statement As at 04-Feb-2020: Print Date: Tuesday, February 4, 2020Document1 pagePolicy Statement As at 04-Feb-2020: Print Date: Tuesday, February 4, 2020Kalyesubula Mahad AraaliNo ratings yet
- Policy Statement As at 04-Apr-2020: Print Date: Saturday, April 4, 2020Document1 pagePolicy Statement As at 04-Apr-2020: Print Date: Saturday, April 4, 2020Kalyesubula Mahad AraaliNo ratings yet
- Lockdown Period Letter To AgentsDocument3 pagesLockdown Period Letter To AgentsKalyesubula Mahad AraaliNo ratings yet
- No - Particulars Qty Unit Amount RemarksDocument3 pagesNo - Particulars Qty Unit Amount RemarksKalyesubula Mahad Araali50% (2)
- Invoice Mahad 15845903984836Document1 pageInvoice Mahad 15845903984836Kalyesubula Mahad AraaliNo ratings yet
- Form of Discharge Surrender Value Benefits Endowment Assurance With Profits (T) - No. 120/eaw/020579Document1 pageForm of Discharge Surrender Value Benefits Endowment Assurance With Profits (T) - No. 120/eaw/020579Kalyesubula Mahad AraaliNo ratings yet
- COVID 19 IRA Release - FINALDocument1 pageCOVID 19 IRA Release - FINALKalyesubula Mahad AraaliNo ratings yet
- Lockdown Period Letter To AgentsDocument3 pagesLockdown Period Letter To AgentsKalyesubula Mahad AraaliNo ratings yet
- Need A Life PolicyDocument1 pageNeed A Life PolicyKalyesubula Mahad AraaliNo ratings yet
- Level3 113022Document6 pagesLevel3 113022kage galang100% (1)
- Updated CVDocument4 pagesUpdated CVcrazylucarioNo ratings yet
- 3D Transthoracic Echocardiography Provides Accurate Cross-Sectional Area of The RV Outflow Tract - 1Document3 pages3D Transthoracic Echocardiography Provides Accurate Cross-Sectional Area of The RV Outflow Tract - 1Thumper KatesNo ratings yet
- U.P. Board of Regents v. Rasul PDFDocument11 pagesU.P. Board of Regents v. Rasul PDFPaolo Antonio EscalonaNo ratings yet
- PMPR - PGY1 International ProgramsDocument2 pagesPMPR - PGY1 International ProgramsFelipe SotoNo ratings yet
- A Study Report On Medical Record DepartmentDocument45 pagesA Study Report On Medical Record Departmentazhar ahmedNo ratings yet
- The Good NurseDocument4 pagesThe Good Nursejannah fadhilahNo ratings yet
- Sami Dalessio-ResumeDocument1 pageSami Dalessio-Resumeapi-405167654No ratings yet
- Prelacrimal Approach To Maxillare SinusesDocument5 pagesPrelacrimal Approach To Maxillare SinusesBagus Sofian AdhatamaNo ratings yet
- CV Nguyen Thanh HuongDocument2 pagesCV Nguyen Thanh HuongAnonymous CB4JU5uaNo ratings yet
- Carotid and Vertebral Ultrasonography - Dr. DanielDocument74 pagesCarotid and Vertebral Ultrasonography - Dr. DanielSuci Rahayu Evasha100% (1)
- Gomes WSES 15Document6 pagesGomes WSES 15zakyNo ratings yet
- 1 s2.0 S1879406821000631 MainDocument1 page1 s2.0 S1879406821000631 MainmiNo ratings yet
- Davina Saltos ResumeDocument1 pageDavina Saltos ResumeDavina SaltosNo ratings yet
- Chest Drains Al-WPS OfficeDocument16 pagesChest Drains Al-WPS OfficeisnainiviaNo ratings yet
- Visa FormsDocument2 pagesVisa FormsAnastasiafynn100% (1)
- Prognosis SampleDocument3 pagesPrognosis SampleCJ GambaNo ratings yet
- Psychiatric Case History: General Instructions: This Model Case History Is Quite Comprehensive. Most Case HistoriesDocument3 pagesPsychiatric Case History: General Instructions: This Model Case History Is Quite Comprehensive. Most Case HistoriesKelly Queenie AndresNo ratings yet
- Verb Tense - StructureDocument3 pagesVerb Tense - Structureapi-179604969No ratings yet
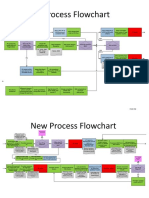
- New Process Flowchart CPOEDocument4 pagesNew Process Flowchart CPOELiza GeorgeNo ratings yet
- Readers Digest April 2015Document146 pagesReaders Digest April 2015herbertjohn24100% (1)
- Part 1 Amadeus ScriptDocument42 pagesPart 1 Amadeus ScriptSergiu VladescuNo ratings yet
- SEASAC Softball Girls Programme 2013Document24 pagesSEASAC Softball Girls Programme 2013falconsnistNo ratings yet
- Leg Med SummerDocument69 pagesLeg Med SummerMichael Angelo MemoracionNo ratings yet
- 2 Paths of Bayer Drug in 80'S - Riskier One Steered Overseas - The New York TimesDocument7 pages2 Paths of Bayer Drug in 80'S - Riskier One Steered Overseas - The New York TimeslvcargniniNo ratings yet
- Elbow Fractures Recovery GuideDocument6 pagesElbow Fractures Recovery GuideAmalia ZofotaNo ratings yet
- Pediatric Clinics Aug 2007Document189 pagesPediatric Clinics Aug 2007api-3723525No ratings yet