You might also like
- Evaluation and Diagnosis of Multiple Sclerosis in Adults - UpToDateDocument45 pagesEvaluation and Diagnosis of Multiple Sclerosis in Adults - UpToDatespritdummyNo ratings yet
- Intrathecal MorphineDocument6 pagesIntrathecal MorphineJoana MoreiraNo ratings yet
- Anesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyDocument8 pagesAnesthesia For Major Urologic Surgery: James O.B. Cockcroft,, Colin B. Berry,, John S. Mcgrath,, Mark O. DaughertyJEFFERSON MUÑOZNo ratings yet
- Liquidos y Electrolitos en CirugiaDocument161 pagesLiquidos y Electrolitos en CirugiaFrancis AbdalaNo ratings yet
- Inhalation AnestheticsDocument28 pagesInhalation AnestheticsAttaufiq IrawanNo ratings yet
- AWARENESS UNDER ANESTHESIA: DEFINITION, TYPES, RISK FACTORS & PREVENTIONDocument27 pagesAWARENESS UNDER ANESTHESIA: DEFINITION, TYPES, RISK FACTORS & PREVENTIONagatakassaNo ratings yet
- Epidural AnesthesiaDocument5 pagesEpidural AnesthesiaImran MukhlessNo ratings yet
- 1.05 (Surgery) General Anesthesia - Airway ManagementDocument3 pages1.05 (Surgery) General Anesthesia - Airway ManagementLeo Mari Go LimNo ratings yet
- General-Anesthesia Part 2Document6 pagesGeneral-Anesthesia Part 2Dianne GalangNo ratings yet
- Joint Replacement Anesthesia ManagementDocument55 pagesJoint Replacement Anesthesia ManagementRaguNo ratings yet
- Managing Difficult Airway in Obstetric AnesthesiaDocument3 pagesManaging Difficult Airway in Obstetric AnesthesiaRoman AureliaNo ratings yet
- CH 46 Complications of AnaesthesiaDocument29 pagesCH 46 Complications of AnaesthesiaChristian LeepoNo ratings yet
- S022 - R04 Service Manual Ec 3890li PDFDocument104 pagesS022 - R04 Service Manual Ec 3890li PDFMiguel DiazNo ratings yet
- Epidural AnalgesiaDocument16 pagesEpidural AnalgesiaspreeasNo ratings yet
- Preoperative Patient Assessment and Management: Roxanne Jeen L. FornollesDocument61 pagesPreoperative Patient Assessment and Management: Roxanne Jeen L. FornollesRyan FornollesNo ratings yet
- Royal College X AnesthesiaDocument66 pagesRoyal College X AnesthesiaManuela CormioNo ratings yet
- New Nursing Diagnoses 2012-2014Document11 pagesNew Nursing Diagnoses 2012-2014CarmenNoemiSantos100% (1)
- Anesthesia For Genitourinary SurgeryDocument76 pagesAnesthesia For Genitourinary SurgeryWenny Eka FildayantiNo ratings yet
- ERAS Guidelines PDFDocument8 pagesERAS Guidelines PDFWadezigNo ratings yet
- Anesthesia PresentationDocument19 pagesAnesthesia PresentationJohnyNo ratings yet
- Post-anesthesia hypotension and hypertension treatmentDocument4 pagesPost-anesthesia hypotension and hypertension treatmentDianne GalangNo ratings yet
- The Aspects of GENE THERAPYDocument12 pagesThe Aspects of GENE THERAPYJasmin Prindiana100% (6)
- Patient Positioning Principles in NeurosurgeryDocument6 pagesPatient Positioning Principles in NeurosurgeryBeni BolngNo ratings yet
- ESICM Guidelines On ARDS 2023Document33 pagesESICM Guidelines On ARDS 2023ctsakalakisNo ratings yet
- Labour Analgesia FinalDocument93 pagesLabour Analgesia Finalsanthiyasandy100% (1)
- DRRR Module 4 5Document4 pagesDRRR Module 4 5kellan lyfeNo ratings yet
- Identification, Prevention and Management of Postpartum HaemorrhageDocument11 pagesIdentification, Prevention and Management of Postpartum HaemorrhageCaitlynNo ratings yet
- Epilepsia en El EmbarazoDocument7 pagesEpilepsia en El EmbarazokellydiazromeroNo ratings yet
- Craniopharyngioma-The Anesthetic, Critical Care and Syrgical Challenges in The Managemnet of CPNDocument5 pagesCraniopharyngioma-The Anesthetic, Critical Care and Syrgical Challenges in The Managemnet of CPNpitriaNo ratings yet
- Controlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewDocument49 pagesControlled Hypotension: Moderator: DR V. Y. Srinivas Presenter: Dr. Ann Susan MathewAnn Susan MathewNo ratings yet
- Anaesthetic Drug Crib Sheet-8Document1 pageAnaesthetic Drug Crib Sheet-8Tiarnán Byrne0% (2)
- BJAEd - Hemorragia Obstetrica 2022Document7 pagesBJAEd - Hemorragia Obstetrica 2022Dragos IonixNo ratings yet
- Effective uterotonics for postpartum hemorrhage preventionDocument13 pagesEffective uterotonics for postpartum hemorrhage preventionNicole Andrea Silva GaeteNo ratings yet
- Neonatal Jaundice NICE Threshold GraphsDocument18 pagesNeonatal Jaundice NICE Threshold GraphsChangNo ratings yet
- SSD Power Loss Protection White Paper LoDocument4 pagesSSD Power Loss Protection White Paper LospritdummyNo ratings yet
- Initial Fluid Resuscitation Guided by The Parkland Formula Leads T - 2023 - BurnDocument8 pagesInitial Fluid Resuscitation Guided by The Parkland Formula Leads T - 2023 - BurnBrenda Serrano LaraNo ratings yet
- Mechanical Ventilation in Obese ICU Patients From Intubation To Extubation PDFDocument8 pagesMechanical Ventilation in Obese ICU Patients From Intubation To Extubation PDFEFE VENo ratings yet
- Coherencia HemodinamicaDocument9 pagesCoherencia HemodinamicaMaritza Alejandra Baeza EricesNo ratings yet
- Anesthesia: A Comprehensive Review (5th Edition)Document1 pageAnesthesia: A Comprehensive Review (5th Edition)brakim23No ratings yet
- Ten Tips To Optimize Weaning and Extubation Success in The Critically IllDocument3 pagesTen Tips To Optimize Weaning and Extubation Success in The Critically IllAurora Barrera100% (1)
- Preoperative Evaluation in The 21st CenturyDocument13 pagesPreoperative Evaluation in The 21st CenturyPaulHerrera0% (1)
- Management of Antithrombotic Therapy For Neuraxial and Peripheral Nerve ProceduresDocument3 pagesManagement of Antithrombotic Therapy For Neuraxial and Peripheral Nerve Proceduresjojobod100% (1)
- Guia 13481Document22 pagesGuia 13481CarmenNo ratings yet
- Management of Cardiogenic ShockDocument15 pagesManagement of Cardiogenic ShockcastillojessNo ratings yet
- CardioplegiaDocument1 pageCardioplegiaapi-541766630No ratings yet
- Anestesia OcularDocument156 pagesAnestesia OcularYazmin Peñaloza RoaNo ratings yet
- Supraclavicular Brachial Plexus BlockDocument2 pagesSupraclavicular Brachial Plexus BlockmagedemanNo ratings yet
- Perioperative Medication Management - UpToDateDocument51 pagesPerioperative Medication Management - UpToDateAlex Kulia100% (1)
- HSA ContinuunDocument35 pagesHSA ContinuunJose DavidNo ratings yet
- Intensive Care Unit (ICU)Document14 pagesIntensive Care Unit (ICU)Luis Ribeiro100% (1)
- Failed Spinal Anaesthesia Mechanisms, Management and PreventionDocument6 pagesFailed Spinal Anaesthesia Mechanisms, Management and Preventiondrhemantt1279No ratings yet
- Evans2021 Article SurvivingSepsisCampaignInternaDocument67 pagesEvans2021 Article SurvivingSepsisCampaignInternaPablo Antonio Cruz VivasNo ratings yet
- Primary Aldosteronism - A Multidimensional SyndromeDocument18 pagesPrimary Aldosteronism - A Multidimensional SyndromeErwin SiahaanNo ratings yet
- Doppler Transcraneal 1Document14 pagesDoppler Transcraneal 1Carmen FandiñoNo ratings yet
- IDSA - Guía de Infección Asociada A Catéter VenosoDocument45 pagesIDSA - Guía de Infección Asociada A Catéter Venosoivonne micoltaNo ratings yet
- Guia Japonesa Manejo de La SepsisDocument38 pagesGuia Japonesa Manejo de La SepsisVlady78No ratings yet
- Anesthesia For Cesarean SectionDocument60 pagesAnesthesia For Cesarean Sectionmaheralrwimi100% (1)
- Anesthetic Consideration in Hypertensive PatientDocument11 pagesAnesthetic Consideration in Hypertensive PatientYosiAsmaraNo ratings yet
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Physiology 20 21 22Document2 pages1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 Physiology 20 21 22rkNo ratings yet
- Update in Anaesthesia PDFDocument64 pagesUpdate in Anaesthesia PDFShabih RazaNo ratings yet
- Technique For Awake Fibre Optic IntubationDocument3 pagesTechnique For Awake Fibre Optic Intubationmonir61No ratings yet
- Monitoreo Hemodinamico FuncionalDocument27 pagesMonitoreo Hemodinamico FuncionalGabriel Lopez MNo ratings yet
- Cierre de ColostomiaDocument9 pagesCierre de ColostomiaWildor Herrera GuevaraNo ratings yet
- D'Amico Risk ClassificationDocument6 pagesD'Amico Risk ClassificationStirNo ratings yet
- EBNDocument22 pagesEBNLouis Ann BautistaNo ratings yet
- Anesthesia For Thymectomy 222Document62 pagesAnesthesia For Thymectomy 222drchandrus100% (1)
- Surgery To MG PatientsDocument10 pagesSurgery To MG PatientsKarrar A. AlShammaryNo ratings yet
- Valvular Heart Disease in Elderly Adults - UpToDateDocument31 pagesValvular Heart Disease in Elderly Adults - UpToDatespritdummyNo ratings yet
- Clinical Manifestations of Myasthenia Gravis - UpToDateDocument14 pagesClinical Manifestations of Myasthenia Gravis - UpToDatespritdummyNo ratings yet
- Contoh COPYRIGHT TugasDocument1 pageContoh COPYRIGHT TugasBenyNoerBackboneNo ratings yet
- Diagnosis of Myasthenia Gravis - UpToDateDocument23 pagesDiagnosis of Myasthenia Gravis - UpToDatespritdummyNo ratings yet
- Chronic Immunosuppressive Therapy For Myasthenia Gravis - UpToDateDocument28 pagesChronic Immunosuppressive Therapy For Myasthenia Gravis - UpToDatespritdummyNo ratings yet
- Read MeDocument1 pageRead MeCelle HufkensNo ratings yet
- d1 PDFDocument288 pagesd1 PDFspritdummyNo ratings yet
- 123 MT 2 EQsDocument2 pages123 MT 2 EQsspritdummyNo ratings yet
- Homework Assignment No. 9: Problem SetDocument5 pagesHomework Assignment No. 9: Problem SetspritdummyNo ratings yet
- Mercedes Benz SUVs and Off-Road Models Offer Leading Traction, Comfort and SafetyDocument5 pagesMercedes Benz SUVs and Off-Road Models Offer Leading Traction, Comfort and SafetyspritdummyNo ratings yet
- How To InstallDocument1 pageHow To InstallspritdummyNo ratings yet
- MV 94 PDFDocument1 pageMV 94 PDFEduardo Alonso Martinez MedinaNo ratings yet
- Lemay 2010 Review of Howard Dully - My L PDFDocument8 pagesLemay 2010 Review of Howard Dully - My L PDFspritdummyNo ratings yet
- Software License Agreement TermsDocument1 pageSoftware License Agreement TermsProdromos MpasmatzisNo ratings yet
- Sumatra Selatan - IndonesiaDocument20 pagesSumatra Selatan - IndonesiaspritdummyNo ratings yet
- Sefat 1Document57 pagesSefat 1spritdummyNo ratings yet
- Windows Codecs RawDocument1 pageWindows Codecs Rawsidfrid00No ratings yet
- Publish To The World: Explore by InterestsDocument7 pagesPublish To The World: Explore by InterestsspritdummyNo ratings yet
- Periodic Table (Crystal Structure) - WikipediaDocument5 pagesPeriodic Table (Crystal Structure) - WikipediaspritdummyNo ratings yet
- Warm White Light Emitting Diodes With Gelatin-Coated Agins /zns Core/Shell Quantum DotsDocument7 pagesWarm White Light Emitting Diodes With Gelatin-Coated Agins /zns Core/Shell Quantum DotsspritdummyNo ratings yet
- IEEE Citation Reference: BooksDocument7 pagesIEEE Citation Reference: BooksHsin-Yun HoNo ratings yet
- Nvidia Graphics Accelerator: User's ManualDocument20 pagesNvidia Graphics Accelerator: User's Manualbg2032No ratings yet
- Attitude, Knowledge, and Perception of Health Workers On Transmission and Prevention of Covid-19 in Federal Medical Centre, Birnin Kebbi, Krbbi StateDocument22 pagesAttitude, Knowledge, and Perception of Health Workers On Transmission and Prevention of Covid-19 in Federal Medical Centre, Birnin Kebbi, Krbbi Stateakinbodewa shegxyNo ratings yet
- Dolo 650 MG (Paracetamol) : Uses, Side Effects, DosageDocument3 pagesDolo 650 MG (Paracetamol) : Uses, Side Effects, DosageRaluca Elena Raluca ElenaNo ratings yet
- Introduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions ManualDocument6 pagesIntroduction To Maternity Pediatric Nursing 6th Edition Leifer Solutions Manuallioneldatfcc12100% (28)
- Graham - A Prospective Study of Physiotherapist Prescribed Community Based Exercise in Inflammatory Peripheral NeuropathyDocument8 pagesGraham - A Prospective Study of Physiotherapist Prescribed Community Based Exercise in Inflammatory Peripheral NeuropathykarinaNo ratings yet
- Subarachnoid Haemorrhage SAHDocument8 pagesSubarachnoid Haemorrhage SAHShum Wing Hei JoanneNo ratings yet
- 5 Tips for Preventing Diabetes with Lifestyle ChangesDocument2 pages5 Tips for Preventing Diabetes with Lifestyle Changesmatindi galawanNo ratings yet
- Form C AuthorizationRequestForm PDFDocument4 pagesForm C AuthorizationRequestForm PDFKalaimani SNo ratings yet
- Approach To The Cat With Upper Respiratory Tract Signs Slides 2023Document49 pagesApproach To The Cat With Upper Respiratory Tract Signs Slides 2023Fran G. KittsteinerNo ratings yet
- An EUA For Casirivimab and ImdevimabDocument3 pagesAn EUA For Casirivimab and ImdevimabAllan FradiqueNo ratings yet
- Professional English For Physical SciencesDocument134 pagesProfessional English For Physical SciencesRavindranathan ArumugamNo ratings yet
- DOHaD and Birth Cohort ResearchDocument3 pagesDOHaD and Birth Cohort ResearchNguyễn Tiến HồngNo ratings yet
- Alcohol Dissertation TopicsDocument4 pagesAlcohol Dissertation TopicsOnlinePaperWriterCanada100% (1)
- Food Safety: in A State of Transformation: Global Thematic ResearchDocument44 pagesFood Safety: in A State of Transformation: Global Thematic Researchsajid waqasNo ratings yet
- Heart Disease in PregnancyDocument56 pagesHeart Disease in PregnancyyandraNo ratings yet
- Paraphrasing Name: Rissa Amalia Class: 1B Student ID: 2001913 N o References Paraphrasing Source Mine 1Document2 pagesParaphrasing Name: Rissa Amalia Class: 1B Student ID: 2001913 N o References Paraphrasing Source Mine 1RISSA AMALIANo ratings yet
- Micro LectureDocument4 pagesMicro LectureJewel OlaezNo ratings yet
- Philippines HIV/AIDS Registry For September 2019Document8 pagesPhilippines HIV/AIDS Registry For September 2019Michael DavidNo ratings yet
- UKN Obstetri Maret 2021Document18 pagesUKN Obstetri Maret 2021anton suponoNo ratings yet
- Drug StudyDocument2 pagesDrug Studykev mondaNo ratings yet
- Periprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDocument8 pagesPeriprosthetic Fractures of The Proximal Femur Beyond The Vancouver ClassificationDavidBeatonComuladaNo ratings yet
- Gardasil 9 Summary of Product CharacteristicsDocument46 pagesGardasil 9 Summary of Product CharacteristicsEllaNo ratings yet
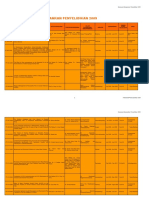
- Data Penyelidikan 2009Document86 pagesData Penyelidikan 2009Alex Phang Kean ChangNo ratings yet
- Health Declaration CardDocument2 pagesHealth Declaration CardJasmin AngieNo ratings yet
- Burn Management Guidelines in EthiopiaDocument28 pagesBurn Management Guidelines in EthiopiaNEsreNo ratings yet
- Syphilis in Pregnancy: Smita Oswal MD DA (UK) MRCA Gordon Lyons MD FRCADocument4 pagesSyphilis in Pregnancy: Smita Oswal MD DA (UK) MRCA Gordon Lyons MD FRCAnur fatinNo ratings yet