You might also like
- Lateral Neck Mass Guide: Pediatric vs. Adult DifferencesDocument62 pagesLateral Neck Mass Guide: Pediatric vs. Adult Differencesசுபத்ரா சந்திரசேகர்No ratings yet
- SGL Case 31 - Study GuideDocument20 pagesSGL Case 31 - Study GuidebangityNo ratings yet
- Atsp Book 2011Document24 pagesAtsp Book 2011Chengyuan ZhangNo ratings yet
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Thyroid UltrasoundDocument9 pagesThyroid UltrasoundMoh SuriyawalNo ratings yet
- Thyroglossal CystsDocument4 pagesThyroglossal CystsCondurache Ilie-AndreiNo ratings yet
- PathologyDocument383 pagesPathology5alifa55No ratings yet
- ThyroidectomyDocument52 pagesThyroidectomyWindelyn Gamaro100% (4)
- Pediatric OSCE A Guide For Medical StudentsDocument9 pagesPediatric OSCE A Guide For Medical Studentsjoey92leeNo ratings yet
- Heart Disease JaninDocument7 pagesHeart Disease JaninTiara Anggun NurartoNo ratings yet
- b17m03l08 Thyroid NodulesDocument11 pagesb17m03l08 Thyroid NodulesJohn Christopher LucesNo ratings yet
- Carpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandCarpal Tunnel Syndrome, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- A Case Presentation On MeningitisDocument29 pagesA Case Presentation On MeningitisNeeta0% (1)
- Colloid Nodular GoiterDocument37 pagesColloid Nodular GoiterLori GeorgeNo ratings yet
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 pagesMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- Neck Mass ProtocolDocument8 pagesNeck Mass ProtocolCharlene FernándezNo ratings yet
- Thyroid Encyclopedia: Encyclopedia of Thyroid Disease, Thyroid Conditions and Thyroid CancerFrom EverandThyroid Encyclopedia: Encyclopedia of Thyroid Disease, Thyroid Conditions and Thyroid CancerNo ratings yet
- Renal colic diagnosis from lab resultsDocument101 pagesRenal colic diagnosis from lab resultsSaad KhanNo ratings yet
- Ultrasound of Thyroid, Parathyroid Glands and Neck Lymph Nodes - SolbiatiDocument14 pagesUltrasound of Thyroid, Parathyroid Glands and Neck Lymph Nodes - Solbiatidrmoscalin8774No ratings yet
- ArtDocument11 pagesArtkarla QuinteroNo ratings yet
- Concept MapDocument9 pagesConcept MapAllene PaderangaNo ratings yet
- Thyroid Nodules and GoiterDocument7 pagesThyroid Nodules and GoiterAgustinaNo ratings yet
- ThyroidCancer Brochure PDFDocument4 pagesThyroidCancer Brochure PDFPutri Juita KhairatihNo ratings yet
- Thyroidectomy: Continuing Education ActivityDocument10 pagesThyroidectomy: Continuing Education Activitybo gum parkNo ratings yet
- Dr. Kunta Setiaji (ThyroidNodule)Document17 pagesDr. Kunta Setiaji (ThyroidNodule)Hasty WahyuniNo ratings yet
- Nontoxic Nodular GoiterDocument9 pagesNontoxic Nodular GoiterKayshey Christine ChuaNo ratings yet
- Solitary Nodules Are Most Likely To Be Malignant in Patients Older Than 60 Years and in Patients Younger Than 30 YearsDocument5 pagesSolitary Nodules Are Most Likely To Be Malignant in Patients Older Than 60 Years and in Patients Younger Than 30 YearsAbdurrahman Afa HaridhiNo ratings yet
- Thyroid Nodules: Clinical PracticeDocument10 pagesThyroid Nodules: Clinical Practicemdowl90No ratings yet
- Thyroid Nodule: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanDocument8 pagesThyroid Nodule: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanRara SafikaNo ratings yet
- Evaluation of thyroid nodules: A risk-stratified approachDocument10 pagesEvaluation of thyroid nodules: A risk-stratified approachAnonymous SjM547DeTNo ratings yet
- Thyroid Cancer: ANATOMY AND PHYSIOLOGY: The Thyroid Is A Butterfly-Shaped Gland That Sits Low OnDocument9 pagesThyroid Cancer: ANATOMY AND PHYSIOLOGY: The Thyroid Is A Butterfly-Shaped Gland That Sits Low OnRitika RanaNo ratings yet
- Thyroid Glands: Kelenjar TiroidDocument3 pagesThyroid Glands: Kelenjar TiroidzieNo ratings yet
- Nontoxic Nodular GoiterDocument7 pagesNontoxic Nodular GoiterKayshey Christine ChuaNo ratings yet
- El Nódulo TiroideoDocument8 pagesEl Nódulo Tiroideoemily peceroNo ratings yet
- BurketsDocument5 pagesBurketssooNo ratings yet
- Safari - 29 Sep 2019 at 21:52Document1 pageSafari - 29 Sep 2019 at 21:52micaNo ratings yet
- Parotid MassDocument9 pagesParotid MassAndre Eka Putra PrakosaNo ratings yet
- Goiter and Thyroid Nodules: Paul W. Ladenson, M.DDocument12 pagesGoiter and Thyroid Nodules: Paul W. Ladenson, M.DFeronicha MaharaniNo ratings yet
- Pathology Lab V Diffuse and Multinodular Goiter.Document18 pagesPathology Lab V Diffuse and Multinodular Goiter.Jeffry Chandra TjahayadiNo ratings yet
- CASE REPORT: TIROID CARCINOMADocument11 pagesCASE REPORT: TIROID CARCINOMAAldy BimaNo ratings yet
- Nodulo TiroideoDocument6 pagesNodulo TiroideoKammiloPalaciosNo ratings yet
- Jurnal OnkologiDocument11 pagesJurnal OnkologiIrham HasbiNo ratings yet
- US Clínica de Glándulas Salivales 2009Document28 pagesUS Clínica de Glándulas Salivales 2009Lucila BrañaNo ratings yet
- Thyroid Nodules: What Is The Thyroid Gland?Document3 pagesThyroid Nodules: What Is The Thyroid Gland?sougataNo ratings yet
- Case BedahDocument16 pagesCase BedahbidiNo ratings yet
- What Is A Thyroid NoduleDocument1 pageWhat Is A Thyroid NodulecartitimiNo ratings yet
- Lecture 46 April 11th-EndocrineDocument3 pagesLecture 46 April 11th-Endocrineapi-26938624No ratings yet
- 01 MNG OcdDocument4 pages01 MNG OcdShopana PeterNo ratings yet
- Thyroid NodulesDocument23 pagesThyroid NodulesPanjtan PakNo ratings yet
- Neck Masses: Guide to Thyroid Disease Diagnosis and TreatmentDocument49 pagesNeck Masses: Guide to Thyroid Disease Diagnosis and TreatmentRashed ShatnawiNo ratings yet
- Thyroid NodulesDocument43 pagesThyroid NodulesRaker AMSANo ratings yet
- Thyroid Nodule PDFDocument21 pagesThyroid Nodule PDFrima oktariniNo ratings yet
- A Case Study In:: Thyroid CancerDocument18 pagesA Case Study In:: Thyroid CancerJaimie La PenaNo ratings yet
- Toxic AdenomaDocument5 pagesToxic AdenomaRayan JabbarNo ratings yet
- الدرقDocument10 pagesالدرقmas2k212No ratings yet
- Case Study: Post-Infectious Hydrocephalus and Indirect Inguinal HerniaDocument24 pagesCase Study: Post-Infectious Hydrocephalus and Indirect Inguinal HerniaArha Mae BaliwasNo ratings yet
- CT Public v82 8 9Document2 pagesCT Public v82 8 9Dida HermaNo ratings yet
- Papillary Thyroid Ca: Group. 1 B Grand CaseDocument16 pagesPapillary Thyroid Ca: Group. 1 B Grand CaseAdora Dela CruzNo ratings yet
- Papillary Thyroid Ca: Group. 1 B Grand CaseDocument16 pagesPapillary Thyroid Ca: Group. 1 B Grand CaseAdora Dela CruzNo ratings yet
- Management of The Thyroid NoduleDocument8 pagesManagement of The Thyroid NoduleJose Tomás MooreNo ratings yet
- Nodulos Tiroideos PDFDocument16 pagesNodulos Tiroideos PDFTay SalinasNo ratings yet
- Laparoscopic AdrenalectomyDocument12 pagesLaparoscopic AdrenalectomyTay SalinasNo ratings yet
- Perspectives On Mechanical Small Bowel Obstruction in AdultsDocument6 pagesPerspectives On Mechanical Small Bowel Obstruction in AdultsTay SalinasNo ratings yet
- Bowel Obstruction s13017-019-0240-7Document8 pagesBowel Obstruction s13017-019-0240-7HadsabsaNo ratings yet
- Bowel Obstruction StatPearlsDocument5 pagesBowel Obstruction StatPearlsTay SalinasNo ratings yet
- Mesenterico PDFDocument7 pagesMesenterico PDFTay SalinasNo ratings yet
- Placental Vascular Pathology and Increased Thrombin Generation As Mechanisms of Disease in Obstetrical SyndromesDocument26 pagesPlacental Vascular Pathology and Increased Thrombin Generation As Mechanisms of Disease in Obstetrical SyndromesTay SalinasNo ratings yet
- Dysphagia: Ahmad S. Ashrafi, and R. Sudhir SundaresanDocument9 pagesDysphagia: Ahmad S. Ashrafi, and R. Sudhir SundaresanTay SalinasNo ratings yet
- Acute Myeloid Leukemia: Advances in Diagnosis and Classi CationDocument9 pagesAcute Myeloid Leukemia: Advances in Diagnosis and Classi CationTay SalinasNo ratings yet
- Estados Alterados de La ConcienciaDocument13 pagesEstados Alterados de La ConcienciaTay SalinasNo ratings yet
- Chapter 22 Streptococcus, Enterococcus and PneumococcusDocument73 pagesChapter 22 Streptococcus, Enterococcus and PneumococcusPriyanshiNo ratings yet
- Chart of Eye SymptomsDocument1 pageChart of Eye SymptomsRaghunandan RamanathanNo ratings yet
- Modified Bar Bending Method of Thoracoscopic NussDocument10 pagesModified Bar Bending Method of Thoracoscopic NussAlfadinAzzahrawaaniElNauvalNo ratings yet
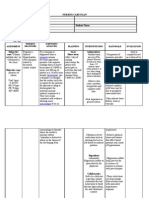
- Nursing Care PlanDocument2 pagesNursing Care PlanDan TijamNo ratings yet
- Investigation of Outbreak 2Document54 pagesInvestigation of Outbreak 2Evan Permana PutraNo ratings yet
- Decubitus Ulcer Wound Care - RefratDocument35 pagesDecubitus Ulcer Wound Care - RefratheraNo ratings yet
- A Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersDocument4 pagesA Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersRiszki_03No ratings yet
- Ptosis: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanDocument13 pagesPtosis: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2019 JanAnonymous LnWIBo1GNo ratings yet
- NCP Risk For Infection TuberculosisDocument3 pagesNCP Risk For Infection TuberculosisWen SilverNo ratings yet
- 5Document47 pages5Nasti PalilingNo ratings yet
- Hepatic Encephalopathy-The Old and The NewDocument19 pagesHepatic Encephalopathy-The Old and The NewWando LunNo ratings yet
- MicroorganismsDocument12 pagesMicroorganismsMiggy GNo ratings yet
- Baby Lab Honors ProjectDocument2 pagesBaby Lab Honors Projectapi-371034570No ratings yet
- Tutorial 1 1. General Learning ObjectiveDocument2 pagesTutorial 1 1. General Learning ObjectiveMartha Marthad.karifoNo ratings yet
- Bone Fracture Types, Causes, Signs and TreatmentDocument23 pagesBone Fracture Types, Causes, Signs and TreatmentGizachew AsimareNo ratings yet
- Taenia saginata and solium: Pathogens Causing CysticercosisDocument20 pagesTaenia saginata and solium: Pathogens Causing CysticercosisfaradillaNo ratings yet
- Hamstring Muscle Injuries - OrthoInfo - AAOSDocument8 pagesHamstring Muscle Injuries - OrthoInfo - AAOSAndy Delos ReyesNo ratings yet
- Respiratory Part 2Document23 pagesRespiratory Part 2api-26938624No ratings yet
- Focal InfectionDocument2 pagesFocal InfectionRoza NafilahNo ratings yet
- Dr. Niroopama Pushpagiri: RSR Sarada Maternity Hospital, Pogathota, NelloreDocument51 pagesDr. Niroopama Pushpagiri: RSR Sarada Maternity Hospital, Pogathota, Nelloresushmanth reddy katamreddyNo ratings yet
- Sepsis: Sepsis and Septic ShockDocument22 pagesSepsis: Sepsis and Septic ShockWialda Dwi rodyahNo ratings yet
- (NEJM, May 2023) - Medication-Related Osteonecrosis of The Jaw (Images in Clinical Medicine)Document1 page(NEJM, May 2023) - Medication-Related Osteonecrosis of The Jaw (Images in Clinical Medicine)NigelyulNo ratings yet
- Drug Study Grand CaseDocument7 pagesDrug Study Grand CaseGel Torres GalvezNo ratings yet
- Imaging of Acute Abdomen in PregnancyDocument18 pagesImaging of Acute Abdomen in Pregnancyshofa nur rahmannisaNo ratings yet
- PIRO Classification Predicts Outcomes in Pediatric SepsisDocument7 pagesPIRO Classification Predicts Outcomes in Pediatric SepsisDiana Paola Castaño SalazarNo ratings yet
- 3rd Mid CaseDocument32 pages3rd Mid CaseHarshini MakkenaNo ratings yet