You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Salmonella Rapid Test: Certest BiotecDocument16 pagesSalmonella Rapid Test: Certest BiotecOlesyaGololobovaNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Mod 1 Student OutlineDocument8 pagesMod 1 Student OutlineOlesyaGololobovaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Hemorrhagic FeverDocument19 pagesHemorrhagic FeverOlesyaGololobovaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Rickettsia Prowazekii: (Epidemic Typhus)Document2 pagesRickettsia Prowazekii: (Epidemic Typhus)OlesyaGololobovaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Bantuan Hidup Dasar: Update of 2020 GuidelinesDocument27 pagesBantuan Hidup Dasar: Update of 2020 GuidelinesRJP Nurse Gaming100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- BSNDocument1 pageBSNAnonymous 75TDy2yNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Pengaruh Aplikasi Karbamid Peroksida 20% Dan 35% Terhadap Kekerasan Resin Komposit Mikro HibridDocument5 pagesPengaruh Aplikasi Karbamid Peroksida 20% Dan 35% Terhadap Kekerasan Resin Komposit Mikro HibridAyasha ApriliaNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Human African Trypanosomiasis Review June 2017Document27 pagesHuman African Trypanosomiasis Review June 2017yeniNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Olanzapine Vs AripiprazoleDocument8 pagesOlanzapine Vs AripiprazoleDivaviyaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Successful Aging and Frailty Opposite Sides of The SameDocument5 pagesSuccessful Aging and Frailty Opposite Sides of The SameGary Xavier Puc CetzNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Health Psychology: Bio Psychosocial Perspective: Ranya Al-Mandawi Dr. Tyrin Stevenson Psych 331Document6 pagesHealth Psychology: Bio Psychosocial Perspective: Ranya Al-Mandawi Dr. Tyrin Stevenson Psych 331Ranya NajiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Unit-I. Epidemiology IntroductionDocument60 pagesUnit-I. Epidemiology IntroductionAny OneNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- CDC Booster RecommendationsDocument21 pagesCDC Booster RecommendationsNational Content DeskNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Surehands LMNDocument1 pageSurehands LMNapi-383151067No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Case Presentation On Recurrent PULMONARY EMBOLISMDocument14 pagesCase Presentation On Recurrent PULMONARY EMBOLISMAkas RehmanNo ratings yet
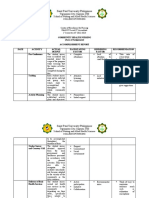
- Group 4 - Accomplishment ReportDocument5 pagesGroup 4 - Accomplishment ReportMa. Millen PagadorNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DLP - Mathematics 2 - Ma. Jasmin BarelaDocument6 pagesDLP - Mathematics 2 - Ma. Jasmin BarelaMa. Jasmin BarelaNo ratings yet
- Project ProposalDocument5 pagesProject ProposalJessica GlitterNo ratings yet
- The Secret To Great Health Escaping The Healthcare Matrix FinalDocument22 pagesThe Secret To Great Health Escaping The Healthcare Matrix FinalpenstyloNo ratings yet
- Disease DetectivesDocument2 pagesDisease DetectivesbkberkowitzNo ratings yet
- 2015 UEMX 3613 Topic4-Risk AssessmentDocument38 pages2015 UEMX 3613 Topic4-Risk AssessmentigantiNo ratings yet
- 10 1 1 115Document151 pages10 1 1 115Angela TorrenteNo ratings yet
- List of Providers - 10032023Document24 pagesList of Providers - 10032023Rodalyn PaddayumanNo ratings yet
- Valencia Medical Hospital: Sayre Highway, Valencia City, BukidnonDocument20 pagesValencia Medical Hospital: Sayre Highway, Valencia City, BukidnonPaula Martina Camille ChioNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Vacant Seats For Transfer - Admissions 2022Document4 pagesVacant Seats For Transfer - Admissions 2022Shahroz RindNo ratings yet
- Cytotoxic Spill Management 1Document3 pagesCytotoxic Spill Management 1pccnursemanager100% (1)
- Secondary Health 7 Q4 Module4Document9 pagesSecondary Health 7 Q4 Module4Rona RuizNo ratings yet
- Un Sustainable Development GoalsDocument3 pagesUn Sustainable Development GoalsChampyNo ratings yet
- Executive Order 202-202.37 (June 05)Document87 pagesExecutive Order 202-202.37 (June 05)OANo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- ATLS PretestDocument3 pagesATLS PretestDavid Reznick100% (5)
- SalmonellaDocument103 pagesSalmonellabrucella2308No ratings yet
- World Medical Association Declaration of HelsinkiDocument5 pagesWorld Medical Association Declaration of Helsinkiapi-3711862No ratings yet
- Advert Gender and Defence 25.04.2023Document18 pagesAdvert Gender and Defence 25.04.2023kingNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)