You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The 15 Most Homeless Cities in The WorldDocument16 pagesThe 15 Most Homeless Cities in The WorldGennaro ThiagoNo ratings yet
- SH Libro CompletoDocument80 pagesSH Libro CompletoMickel Caballero100% (1)
- Piping Class: PROJ: 2963 REV: 1 DOC: PPAG-100-ET-C-009Document5 pagesPiping Class: PROJ: 2963 REV: 1 DOC: PPAG-100-ET-C-009Santiago GarciaNo ratings yet
- Bemco Steel Industries Co. LTD.: Qp10-Q-6764 - Typicalsteelwatertower1500MDocument12 pagesBemco Steel Industries Co. LTD.: Qp10-Q-6764 - Typicalsteelwatertower1500MhgagNo ratings yet
- Hydraulic Rock Drill He 122: Serial NumberDocument6 pagesHydraulic Rock Drill He 122: Serial NumberElizabeth OctagonNo ratings yet
- Kenmore 385.17624 Sewing Machine Instruction ManualDocument109 pagesKenmore 385.17624 Sewing Machine Instruction ManualiliiexpugnansNo ratings yet
- Wasonga's PaperDocument13 pagesWasonga's PaperWillis WasongaNo ratings yet
- Textbook Marina Carr Pastures of The Unknown Melissa Sihra Ebook All Chapter PDFDocument53 pagesTextbook Marina Carr Pastures of The Unknown Melissa Sihra Ebook All Chapter PDFcharles.valle114100% (10)
- Mechanical Engineering Syllabus at The Amrita Vishwa Vidyapeetham, Coimbatore CampusDocument3 pagesMechanical Engineering Syllabus at The Amrita Vishwa Vidyapeetham, Coimbatore CampusMathan76No ratings yet
- XTRACT Fall2012 Manual PDFDocument15 pagesXTRACT Fall2012 Manual PDFJuan Pablo PeñalosaNo ratings yet
- Canon Option Platen Cover Type S PC Rev0 100312Document16 pagesCanon Option Platen Cover Type S PC Rev0 100312Jaime RiosNo ratings yet
- Ch. 5 - No Future For White MenDocument29 pagesCh. 5 - No Future For White MenEleanora LawrenceNo ratings yet
- Balochistan Public Procurement Rules 2014Document41 pagesBalochistan Public Procurement Rules 2014Muhammad AzamNo ratings yet
- Clio2 Groupen en PDFDocument57 pagesClio2 Groupen en PDFAlexandru TerciuNo ratings yet
- Project ApolloDocument174 pagesProject ApolloSpil_vv_IJmuiden100% (1)
- 9a L5 Vocab NotesDocument7 pages9a L5 Vocab NotesCindy NguyenNo ratings yet
- Chapter 1 Practice Quiz PrintoutDocument2 pagesChapter 1 Practice Quiz PrintoutlisajleanbalNo ratings yet
- Customize Your Parfait Pen National Pen PDFDocument1 pageCustomize Your Parfait Pen National Pen PDFMary MptNo ratings yet
- Nguyen Thi Thu Thao: ExperienceDocument2 pagesNguyen Thi Thu Thao: ExperienceThao NguyenNo ratings yet
- Switchgear Vs SwitchboardDocument20 pagesSwitchgear Vs SwitchboardJuan MoralesNo ratings yet
- Interactive Schematic: This Document Is Best Viewed at A Screen Resolution of 1024 X 768Document32 pagesInteractive Schematic: This Document Is Best Viewed at A Screen Resolution of 1024 X 768CarlosNo ratings yet
- Ime 100l Mcaxr0100eab LowDocument4 pagesIme 100l Mcaxr0100eab LowVictorNo ratings yet
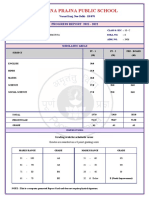
- Poorna Prajna Public School: Progress Report 2021 - 2022Document1 pagePoorna Prajna Public School: Progress Report 2021 - 2022SwagBeast SKJJNo ratings yet
- E3-282 MidSemPaper Aug2021Document3 pagesE3-282 MidSemPaper Aug2021Wiluam Rutherford BondNo ratings yet
- SG-CR01: Contact Person: Mr. Wonder Mobile: +86 15158106703 Tel: +86 571 63131356 Skype: WonderofficeworksDocument2 pagesSG-CR01: Contact Person: Mr. Wonder Mobile: +86 15158106703 Tel: +86 571 63131356 Skype: WonderofficeworksШеф ОтрисовкаNo ratings yet
- Hypnosis OusbyDocument51 pagesHypnosis OusbyRazvan Popadiuc100% (8)
- III AssociateDocument2 pagesIII Associateagupta_118177No ratings yet
- Congruence Model: Submitted By-SyndicateDocument9 pagesCongruence Model: Submitted By-SyndicateKrishnakant NeekhraNo ratings yet
- Overcoming Apathy and Classroom Disconnect in Marketing Courses: Employing Karaoke Jeopardy As A Content Retention ToolDocument7 pagesOvercoming Apathy and Classroom Disconnect in Marketing Courses: Employing Karaoke Jeopardy As A Content Retention ToolNATALY MISHELLE ROSERO HERRERANo ratings yet
- Sor - WRD Gob - 01 - 10 - 12Document383 pagesSor - WRD Gob - 01 - 10 - 12Abhishek sNo ratings yet