You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 1 FCRDocument1 page1 FCRLuis GómezNo ratings yet
- Posterior Cortical Atrophy Patients Present with Visual ImpairmentDocument5 pagesPosterior Cortical Atrophy Patients Present with Visual ImpairmentLuis GómezNo ratings yet
- Consensus Classification of Posterior Cortical AtrDocument15 pagesConsensus Classification of Posterior Cortical AtrLuis GómezNo ratings yet
- Peña-Casanova, J., et al. (2009). Spanish Multicenter Normative Studies (NEURONORMA Project). Norms for the Rey–Osterrieth Complex Figure (Copy and Memory), and Free and Cued Selective Reminding TestDocument23 pagesPeña-Casanova, J., et al. (2009). Spanish Multicenter Normative Studies (NEURONORMA Project). Norms for the Rey–Osterrieth Complex Figure (Copy and Memory), and Free and Cued Selective Reminding TestLuis GómezNo ratings yet
- Regional EEG Changes Reflect Visual Deficits in PCADocument11 pagesRegional EEG Changes Reflect Visual Deficits in PCALuis GómezNo ratings yet
- Supplementary Figure 1. Negligible Effects of Covarying For Different Tracer Injection ParametersDocument6 pagesSupplementary Figure 1. Negligible Effects of Covarying For Different Tracer Injection ParametersLuis GómezNo ratings yet
- (Macaulay, M. & Macmillan, M.) The Concept of Mental Age and MaturationDocument4 pages(Macaulay, M. & Macmillan, M.) The Concept of Mental Age and MaturationLuis GómezNo ratings yet
- Posterior Cortical Atrophy Patients Present with Visual ImpairmentDocument5 pagesPosterior Cortical Atrophy Patients Present with Visual ImpairmentLuis GómezNo ratings yet
- Genetics and Epigenetics of Autism Spectrum DisorderDocument11 pagesGenetics and Epigenetics of Autism Spectrum DisorderPAULANo ratings yet
- (Zimmerman, D., Et Al.) Independence of Hot and Cold Executive Function Deficits in High - Functioning Adults With Autism Spectrum DisorderDocument15 pages(Zimmerman, D., Et Al.) Independence of Hot and Cold Executive Function Deficits in High - Functioning Adults With Autism Spectrum DisorderLuis GómezNo ratings yet
- (Greenspan, N.) Autism, Evolution, and The Inadequacy of SpectrumDocument4 pages(Greenspan, N.) Autism, Evolution, and The Inadequacy of SpectrumLuis GómezNo ratings yet
- BOT-2 Complete Form Sample Report PDFDocument12 pagesBOT-2 Complete Form Sample Report PDFmarioh_40% (1)
- The 2D:4D Ratio and Its Relationship With Other Androgenisation Parameters in Parents of Individuals With Autism Spectrum DisordersDocument8 pagesThe 2D:4D Ratio and Its Relationship With Other Androgenisation Parameters in Parents of Individuals With Autism Spectrum DisordersLuis GómezNo ratings yet
- Author's Accepted Manuscript: Psychiatry ResearchDocument29 pagesAuthor's Accepted Manuscript: Psychiatry ResearchLuis GómezNo ratings yet
- Anak Coba ImiDocument18 pagesAnak Coba ImiMarchelina Benediktin KaunangNo ratings yet
- Emerging Framework for Understanding Cognition Through Large-Scale Brain NetworksDocument14 pagesEmerging Framework for Understanding Cognition Through Large-Scale Brain NetworksLuis GómezNo ratings yet
- (Mizuno, Y., Et Al.) Structural Brain Abnormalities in ChildrenDocument7 pages(Mizuno, Y., Et Al.) Structural Brain Abnormalities in ChildrenLuis GómezNo ratings yet
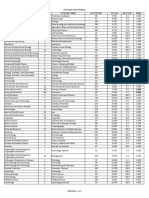
- Annual Review Of: in Category Category Name in Category Factor Half-Life IndexDocument2 pagesAnnual Review Of: in Category Category Name in Category Factor Half-Life IndexLuis GómezNo ratings yet
- Aging and Alzheimer'S Disease: Lessons From The Nun Study: David A. Snowdon, PHDDocument7 pagesAging and Alzheimer'S Disease: Lessons From The Nun Study: David A. Snowdon, PHDLuis GómezNo ratings yet
- (Revisión) The Cognitive-Affective Neuroscience of The Unconscious (Stein, D., Et Al.)Document5 pages(Revisión) The Cognitive-Affective Neuroscience of The Unconscious (Stein, D., Et Al.)Luis GómezNo ratings yet
- Bruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOT-2)Document2 pagesBruininks-Oseretsky Test of Motor Proficiency, Second Edition (BOT-2)Luis GómezNo ratings yet
- Mapping The Network For PlanningDocument15 pagesMapping The Network For PlanningLuis GómezNo ratings yet
- Psychiatric Adverse Drug Reactions in The Paediatric PopulationDocument7 pagesPsychiatric Adverse Drug Reactions in The Paediatric PopulationLuis GómezNo ratings yet
- DualTask Performance in Dysexecutive and Nondysexecutive Patients With A Frontal LesionDocument8 pagesDualTask Performance in Dysexecutive and Nondysexecutive Patients With A Frontal LesionLuis GómezNo ratings yet
- Zylowska2007 PDFDocument11 pagesZylowska2007 PDFLuis GómezNo ratings yet
- (Wilson, H., Et Al.) Imidazoline 2 Binding Sites Reflecting Astroglia Pathology in Parkinson's Disease. An in Vivo 11CBU99008 PET Study PDFDocument13 pages(Wilson, H., Et Al.) Imidazoline 2 Binding Sites Reflecting Astroglia Pathology in Parkinson's Disease. An in Vivo 11CBU99008 PET Study PDFLuis GómezNo ratings yet
- Caracteristicas Fisicas y Fenotipo Conductual - Galvan Manso y Otros - ArticuloDocument5 pagesCaracteristicas Fisicas y Fenotipo Conductual - Galvan Manso y Otros - ArticuloPedro Fernández CardellaNo ratings yet
- Mapping The Network For PlanningDocument15 pagesMapping The Network For PlanningLuis GómezNo ratings yet
- (Cohen, A. Et Al.) Looking Beyond The Face Area. Lesion Network Mapping of Prosopagnosia PDFDocument16 pages(Cohen, A. Et Al.) Looking Beyond The Face Area. Lesion Network Mapping of Prosopagnosia PDFLuis GómezNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- National Guidelines For Management of Covid-19Document203 pagesNational Guidelines For Management of Covid-19African Centre for Media ExcellenceNo ratings yet
- Mood Disorders: Dr. C. George BoereeDocument5 pagesMood Disorders: Dr. C. George Boereefemfen1225No ratings yet
- Non Operative Treatment Is A Reliable Option in Over T 2019 Orthopaedics TDocument6 pagesNon Operative Treatment Is A Reliable Option in Over T 2019 Orthopaedics TdrelvNo ratings yet
- Study of Rate, Cause and Pattern of Hospital Readmissions in Emergency Medicine of A Tertiary Care Hospital in North IndiaDocument7 pagesStudy of Rate, Cause and Pattern of Hospital Readmissions in Emergency Medicine of A Tertiary Care Hospital in North IndiaIJAR JOURNALNo ratings yet
- Medication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsDocument10 pagesMedication Adherence and Blood Pressure Control Among Hypertensive Patients With Coexisting Long-Term Conditions in Primary Care SettingsmadhurocksktmNo ratings yet
- Vanderlind - 2021Document14 pagesVanderlind - 2021Sergio GarcíaNo ratings yet
- Abdii The LastDocument51 pagesAbdii The Lastdaniel mitikuNo ratings yet
- NTCC Srishti K 144Document16 pagesNTCC Srishti K 144srishti kohliNo ratings yet
- Folliculitis Decalvans Effectiveness of Therapies and Prognostic Factors in A Multicenter Series of 60 Patients With Long Term Follow UpDocument6 pagesFolliculitis Decalvans Effectiveness of Therapies and Prognostic Factors in A Multicenter Series of 60 Patients With Long Term Follow Upabdulmunim hanyNo ratings yet
- DhatDocument11 pagesDhatLetterio NaccariNo ratings yet
- School Based Mental Health and Psychosocial Wellness in the PhilippinesDocument89 pagesSchool Based Mental Health and Psychosocial Wellness in the PhilippinesOliv KrisNo ratings yet
- Godi Szilard PHD DolgozatDocument103 pagesGodi Szilard PHD DolgozatHry EzaNo ratings yet
- Atomoxetine in ADHD in Children With and Without Comorbid Mood DisordersDocument10 pagesAtomoxetine in ADHD in Children With and Without Comorbid Mood DisordersNeuro GYMNo ratings yet
- Relationship of Care Giver and Their PatientDocument39 pagesRelationship of Care Giver and Their PatientGunawan iriantoNo ratings yet
- ACL Reconstruction ProtocolDocument2 pagesACL Reconstruction ProtocolyaasarloneNo ratings yet
- BPD MagazineDocument92 pagesBPD Magazinetan hangNo ratings yet
- Journal of Internal Medicine - 2019 - Shaw - The Face of Postural Tachycardia Syndrome Insights From A Large 2Document11 pagesJournal of Internal Medicine - 2019 - Shaw - The Face of Postural Tachycardia Syndrome Insights From A Large 2Liza HavengaNo ratings yet
- Dutch Cardiac Rehabilitation Physiotherapy Guidelines PDFDocument52 pagesDutch Cardiac Rehabilitation Physiotherapy Guidelines PDFyohanNo ratings yet
- Fact Sheet InterQual Criteria PortfolioDocument4 pagesFact Sheet InterQual Criteria PortfolioMora MDNo ratings yet
- Nurs 3021 SiloDocument5 pagesNurs 3021 Siloapi-642843871No ratings yet
- Alexander Müller (Sildenafil)Document5 pagesAlexander Müller (Sildenafil)Antonio SanchezNo ratings yet
- Abu Dhabi DRGDocument62 pagesAbu Dhabi DRGDolly creationsNo ratings yet
- MSF OCA NCD Guidelines v3 2018Document139 pagesMSF OCA NCD Guidelines v3 2018PepepottNo ratings yet
- A Brief Measure of Worry Severity (BMWS)Document16 pagesA Brief Measure of Worry Severity (BMWS)volglmNo ratings yet
- Test Bank For Abnormal Psychology 17th Edition 17th EditionDocument55 pagesTest Bank For Abnormal Psychology 17th Edition 17th EditionJanice Linder100% (31)
- NURS-FPX6026 - WhitneyPierre - Assessment 3-1docxDocument6 pagesNURS-FPX6026 - WhitneyPierre - Assessment 3-1docxCaroline AdhiamboNo ratings yet
- NeurologiaDocument216 pagesNeurologiaPietro BracagliaNo ratings yet
- 2020 Nemeroff - DeP ReviewDocument15 pages2020 Nemeroff - DeP Reviewnermal93No ratings yet
- Prevalence and Types of AnemiaDocument11 pagesPrevalence and Types of AnemiaRossilawati RachmaNo ratings yet
- Outpatient Parenteral Antibiotic Therapy (OPAT) and Inpatient Treatment Strategies For Emergency Department Patients With Cellulitis: A Cost AnalysisDocument9 pagesOutpatient Parenteral Antibiotic Therapy (OPAT) and Inpatient Treatment Strategies For Emergency Department Patients With Cellulitis: A Cost AnalysissesiaNo ratings yet