You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (843)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 3.anaesthesia and Analgesia in ObstetricsDocument7 pages3.anaesthesia and Analgesia in ObstetricsVeena DalmeidaNo ratings yet
- Tugas Akhir Jurnal QodrunnadaDocument34 pagesTugas Akhir Jurnal QodrunnadaAnonymous 2CvtIRVNo ratings yet
- Dokumen - Tips - Daftar Obat KlinikDocument9 pagesDokumen - Tips - Daftar Obat KlinikIke Annisa YuwelzaNo ratings yet
- Discharge Instruction: Fitriani Pratiwi M.PDDocument13 pagesDischarge Instruction: Fitriani Pratiwi M.PDSaniaNo ratings yet
- Intravenous Drug AdministrationDocument33 pagesIntravenous Drug Administrationleiann_jessicaNo ratings yet
- Role of Radiation Oncology in Modern Multidisciplinary Cancer Treatment - PMCDocument20 pagesRole of Radiation Oncology in Modern Multidisciplinary Cancer Treatment - PMCRalf Kevin Piano,RMTNo ratings yet
- Topic 9. Non-Linear PKDocument17 pagesTopic 9. Non-Linear PKjoseNo ratings yet
- Daftar Obat Menurut FI IIIDocument6 pagesDaftar Obat Menurut FI IIIBillyNo ratings yet
- Current Perspective On Nasal Delivery Systems For Chronic RhinosinusitisDocument20 pagesCurrent Perspective On Nasal Delivery Systems For Chronic RhinosinusitisiliyasNo ratings yet
- DosesDocument16 pagesDosesAli Adnan AfridiNo ratings yet
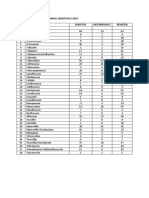
- Peta Antibiotika Rsud Bangil Semester Ii 2018 NO. Jenis Antibiotika ResistenDocument2 pagesPeta Antibiotika Rsud Bangil Semester Ii 2018 NO. Jenis Antibiotika Resistenpkpo dktNo ratings yet
- Nda Fees Regulations 2022 1Document16 pagesNda Fees Regulations 2022 1mulondo abubakerNo ratings yet
- ErcefloraDocument2 pagesErcefloraxtianeduardNo ratings yet
- Department of Physics Department of Physics Department of PhysicsDocument235 pagesDepartment of Physics Department of Physics Department of Physicstatis reyesNo ratings yet
- Hospital Formulary: BY Mrs. K.Shailaja., M. Pharm., Lecturer Dept of Pharmacy Practice, SRM College of PharmacyDocument12 pagesHospital Formulary: BY Mrs. K.Shailaja., M. Pharm., Lecturer Dept of Pharmacy Practice, SRM College of PharmacyDiwya KumarNo ratings yet
- Research MamayaDocument62 pagesResearch MamayaPang ChixxNo ratings yet
- 1 XXX 6Document105 pages1 XXX 6joelrequenaNo ratings yet
- 909-Hazardous Drugs Table - EviqDocument9 pages909-Hazardous Drugs Table - EviqMd Al AminNo ratings yet
- PHARM PAST MCQ AnsweredDocument10 pagesPHARM PAST MCQ AnsweredPrincewill SeiyefaNo ratings yet
- Soal Hitungan DosisDocument2 pagesSoal Hitungan DosissabrinaNo ratings yet
- 01 Airway Management and ProceduresDocument18 pages01 Airway Management and ProceduresChing BanagNo ratings yet
- PSIHOTROPE PARTEA I Bromură de SodiuDocument3 pagesPSIHOTROPE PARTEA I Bromură de SodiuDorel NorocNo ratings yet
- Drug StudyDocument15 pagesDrug StudyDavid RefuncionNo ratings yet
- AnxiolyticsDocument10 pagesAnxiolyticsSharon PanaderoNo ratings yet
- In F Circ ManualDocument4 pagesIn F Circ Manualalexa cuevasNo ratings yet
- ICALL's Crowdsourced List of Mental Health Professionals We Can Trust (23rd April 2021)Document151 pagesICALL's Crowdsourced List of Mental Health Professionals We Can Trust (23rd April 2021)rekhak298No ratings yet
- AR - Stelara (Ustekinumab)Document161 pagesAR - Stelara (Ustekinumab)Ndhy Pharm HabibieNo ratings yet
- UTI Discharge PlanDocument2 pagesUTI Discharge Plankimglaidyl bontuyanNo ratings yet
- Summary of Product Characteristics: 4.1 Therapeutic IndicationsDocument3 pagesSummary of Product Characteristics: 4.1 Therapeutic IndicationsasdwasdNo ratings yet
- Cannabinoid Hyperemesis SyndromeDocument13 pagesCannabinoid Hyperemesis SyndromeDarlene PiperNo ratings yet