You might also like
- Oral Hairy Leukoplakia As A Sign of HIV InfectionDocument5 pagesOral Hairy Leukoplakia As A Sign of HIV InfectionFitri AngginiNo ratings yet
- Oral Hairy LeukplakiaDocument5 pagesOral Hairy LeukplakiarizkiaNo ratings yet
- Hairy LeukoplakiaDocument2 pagesHairy LeukoplakiaEka Septariana PuspaNo ratings yet
- Oral Hairy Leukoplakia: Clinical Indicator of An Immunosuppressive Condition and Challenges in Patient ManagementDocument5 pagesOral Hairy Leukoplakia: Clinical Indicator of An Immunosuppressive Condition and Challenges in Patient ManagementyumizoneNo ratings yet
- Herpes Simplex Virus and Human Papillomavirus Coinfections in Hyperimmunoglobulin E Syndrome Presenting As A Conjunctival Mass LesionDocument5 pagesHerpes Simplex Virus and Human Papillomavirus Coinfections in Hyperimmunoglobulin E Syndrome Presenting As A Conjunctival Mass LesionWalid AissaNo ratings yet
- Erythema Multiforme Associated With Herpes Simplex Virus: A Case Report and Literature ReviewDocument4 pagesErythema Multiforme Associated With Herpes Simplex Virus: A Case Report and Literature ReviewRiza Yanuar RenastyoNo ratings yet
- 9211 - Case ReportDocument4 pages9211 - Case ReportFitri AngginiNo ratings yet
- ADAFlossyGenCrossword EngDocument3 pagesADAFlossyGenCrossword Englisa.prihastariNo ratings yet
- Pathogenesis & Prognosis LeukoplakiaDocument4 pagesPathogenesis & Prognosis LeukoplakiaSundhias LarashatiNo ratings yet
- Mainville 2015Document9 pagesMainville 2015Weslay Rodrigues da SilvaNo ratings yet
- Painful MucosalUlcerations inaPatientWithHIVDocument2 pagesPainful MucosalUlcerations inaPatientWithHIVAndrés MontalvoNo ratings yet
- Admin A 10 1 168 Cd5e504Document5 pagesAdmin A 10 1 168 Cd5e504Bara Bagus RamandaNo ratings yet
- IDTM 2015 24 E132 P.M. 3108Document3 pagesIDTM 2015 24 E132 P.M. 3108Andreas RonaldNo ratings yet
- The Epidemiology of Infections Caused by Escherichia ColiDocument39 pagesThe Epidemiology of Infections Caused by Escherichia ColiTalita ColomeuNo ratings yet
- Pi Is 1875957213001903Document5 pagesPi Is 1875957213001903eppy syafriNo ratings yet
- Chronic Invasive Fungal Sinusitis With Negative Histopathology: A Diagnostic ChallengeDocument4 pagesChronic Invasive Fungal Sinusitis With Negative Histopathology: A Diagnostic ChallengeeshanikasathyaNo ratings yet
- Acute Appendicitis As A Complication of Varicella: Case ReportDocument3 pagesAcute Appendicitis As A Complication of Varicella: Case ReportAngel AdileNo ratings yet
- Hairy Leukoplakia As An Early OralDocument4 pagesHairy Leukoplakia As An Early OralJessicaLisaNugrohoNo ratings yet
- Biology and Disease Associations of Epstein Barr Virus: Dorothy H. CrawfordDocument14 pagesBiology and Disease Associations of Epstein Barr Virus: Dorothy H. CrawfordSabrina ParenteNo ratings yet
- Original Paper: The Study of Uropathogenicity Factors For Escherichia Coli StrainsDocument7 pagesOriginal Paper: The Study of Uropathogenicity Factors For Escherichia Coli StrainsRaluca AdnNo ratings yet
- Bahan Paper PatoDocument6 pagesBahan Paper PatoKhairul Ihsan Pengusaha MudaNo ratings yet
- KNF Jurnal ReadingDocument6 pagesKNF Jurnal ReadingStanislaus Stanley SuhermanNo ratings yet
- Crup Edpidemiologia 3Document5 pagesCrup Edpidemiologia 3Carolina Mora RuedaNo ratings yet
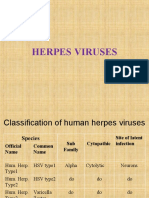
- Herpes VirusesDocument3 pagesHerpes Virusesterah debuyanNo ratings yet
- 1 s2.0 S0213005X19302101Document3 pages1 s2.0 S0213005X19302101A MFNo ratings yet
- Orallesionsassociatedwith Humanimmunodeficiencyvirus DiseaseDocument26 pagesOrallesionsassociatedwith Humanimmunodeficiencyvirus DiseaseGABYZTNo ratings yet
- Lichenoid Skin Lesions - A Rare Manifestation in Secondary SyphilisDocument3 pagesLichenoid Skin Lesions - A Rare Manifestation in Secondary SyphilisShintaNo ratings yet
- Anemia Tasker2002hemobartonellaDocument9 pagesAnemia Tasker2002hemobartonellaOlga Lucia Duque QuijanoNo ratings yet
- Classification of Oral Lesions Associated With HIV Infectionclassification of Oral Lesions Associated With HIV InfectionDocument4 pagesClassification of Oral Lesions Associated With HIV Infectionclassification of Oral Lesions Associated With HIV InfectionHesbon MomanyiNo ratings yet
- HIV-associated Salivary Gland Enlargement: A Clinical ReviewDocument4 pagesHIV-associated Salivary Gland Enlargement: A Clinical ReviewSumayyah EbrahimNo ratings yet
- Howard2019 PDFDocument3 pagesHoward2019 PDFNazihan Safitri AlkatiriNo ratings yet
- MCQ FMS 4 (2016) With AnswersDocument13 pagesMCQ FMS 4 (2016) With Answersstella pangestikaNo ratings yet
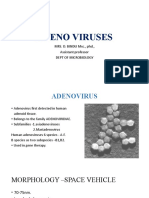
- Adeno Viruses: MRS. D. BINDU MSC., PHD., Assistant Professor Dept of MicrobiologyDocument10 pagesAdeno Viruses: MRS. D. BINDU MSC., PHD., Assistant Professor Dept of Microbiologybindu dhanapalNo ratings yet
- Bégon 2010Document2 pagesBégon 2010pamela queirozNo ratings yet
- 269 FullDocument15 pages269 Fullmurti_fatiyaNo ratings yet
- Secondary SyphilisDocument6 pagesSecondary SyphilisanatomimanusiaNo ratings yet
- Hepatitis Infection: An UpdateDocument48 pagesHepatitis Infection: An UpdateManuel CastilloNo ratings yet
- HERPESVIRUSES, PARVO 2021 Students - KopieDocument38 pagesHERPESVIRUSES, PARVO 2021 Students - KopieMr.FantasthiccNo ratings yet
- Chronic Indolent Orofacial HSV in Chronic LeukemiaDocument4 pagesChronic Indolent Orofacial HSV in Chronic LeukemiaNatalia RafaelNo ratings yet
- Pic RenderDocument5 pagesPic RenderSylvia YuanitaNo ratings yet
- Oral Manifestations of HIV Infection in Adult Patients From The Province of Sancti Spiritus, CubaDocument6 pagesOral Manifestations of HIV Infection in Adult Patients From The Province of Sancti Spiritus, CubaBimalKrishnaNo ratings yet
- Infection MCQDocument49 pagesInfection MCQalh basharNo ratings yet
- Papi LomaDocument10 pagesPapi LomaIsai LVazquezNo ratings yet
- KROK 1 EXPLANATIONS MicrobiologyDocument18 pagesKROK 1 EXPLANATIONS MicrobiologyAkpene Racheal100% (1)
- Abeb QstionsDocument27 pagesAbeb QstionsmphamedNo ratings yet
- Anogenital Warts - An Overview: Devinder Mohan Thappa, M Senthilkumar, Chandrashekar LaxmishaDocument12 pagesAnogenital Warts - An Overview: Devinder Mohan Thappa, M Senthilkumar, Chandrashekar LaxmishaSuci Triana PutriNo ratings yet
- HEV StudyDocument12 pagesHEV StudyjackalackaNo ratings yet
- Feline Herpes Virus-1 Associated Facial and Perianal Dermatitis in A CatDocument4 pagesFeline Herpes Virus-1 Associated Facial and Perianal Dermatitis in A CatIndah frysay marbunNo ratings yet
- Ebv CMVDocument29 pagesEbv CMVSona SandiNo ratings yet
- 1 s2.0 S0168170212004182 MainDocument11 pages1 s2.0 S0168170212004182 MainIon CorbuNo ratings yet
- Allgoewer Et Al-2001-Veterinary OphthalmologyDocument6 pagesAllgoewer Et Al-2001-Veterinary OphthalmologyRose CavalcanteNo ratings yet
- Epstein-Barr Virus (EBV) Infection, Pathogenesis, Diagnosis and EpidemiologyDocument7 pagesEpstein-Barr Virus (EBV) Infection, Pathogenesis, Diagnosis and Epidemiologyميمونه عبد الرحيم مصطفىNo ratings yet
- Cohen2000 Ebv GeralDocument12 pagesCohen2000 Ebv GeralSabrina ParenteNo ratings yet
- Corroboration of A Major Role For Herpes Simplex Virus Type 1 in Alzheimer's DiseaseDocument11 pagesCorroboration of A Major Role For Herpes Simplex Virus Type 1 in Alzheimer's DiseaseMOHAMMAD NAZMUL ISLAMNo ratings yet
- Pathogenesis and Pathology of Lymphatic FilariasisDocument12 pagesPathogenesis and Pathology of Lymphatic Filariasisdies100% (1)
- MCQSseqs Virology - Parstilogy Mycology 2017-1Document8 pagesMCQSseqs Virology - Parstilogy Mycology 2017-1hassan qureshiNo ratings yet
- Medicina 58 00840 v2Document7 pagesMedicina 58 00840 v2elsy oktaviaNo ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Bab 27 Bagian IIDocument8 pagesBab 27 Bagian IIyumizoneNo ratings yet
- Management of Oral Leukoplakia - Analysis of The Literature: Material and MethodsDocument10 pagesManagement of Oral Leukoplakia - Analysis of The Literature: Material and MethodsyunisaNo ratings yet
- Management of Oral Leukoplakia - Analysis of The Literature: Material and MethodsDocument10 pagesManagement of Oral Leukoplakia - Analysis of The Literature: Material and MethodsyunisaNo ratings yet
- Hairy Leukoplakia As An Early OralDocument4 pagesHairy Leukoplakia As An Early OralJessicaLisaNugrohoNo ratings yet
- YmphangioDocument10 pagesYmphangioyumizoneNo ratings yet
- 188 6 883 PDFDocument8 pages188 6 883 PDFyumizoneNo ratings yet
- 188 6 883 PDFDocument8 pages188 6 883 PDFyumizoneNo ratings yet
- The Mcmaster Pediatric Curriculum: at NightDocument39 pagesThe Mcmaster Pediatric Curriculum: at NightyumizoneNo ratings yet
- Bab 7. Struktur KulitDocument56 pagesBab 7. Struktur KulityumizoneNo ratings yet
- PT Estetika Pro International Offers Affordable Aesthetic DevicesDocument9 pagesPT Estetika Pro International Offers Affordable Aesthetic DevicesyumizoneNo ratings yet
- Fitzpatrick Dermatology 8th Ed ASLI (Diseret)Document47 pagesFitzpatrick Dermatology 8th Ed ASLI (Diseret)yumizoneNo ratings yet
- Review: Syphilis and HIV: A Dangerous CombinationDocument11 pagesReview: Syphilis and HIV: A Dangerous CombinationyumizoneNo ratings yet
- Syphilis Increases HIV Viral Load and de PDFDocument5 pagesSyphilis Increases HIV Viral Load and de PDFyumizoneNo ratings yet
- Chapter 112 Ultraviolet Radiation CarcinogenesisDocument17 pagesChapter 112 Ultraviolet Radiation CarcinogenesisyumizoneNo ratings yet
- Seronegative Secondary Syphilis in an HIV PatientDocument3 pagesSeronegative Secondary Syphilis in an HIV PatientyumizoneNo ratings yet
- PPK Perdoski 2017 Skabies (English)Document3 pagesPPK Perdoski 2017 Skabies (English)yumizoneNo ratings yet
- Will Is 2001Document6 pagesWill Is 2001yumizoneNo ratings yet
- Bab 7. Struktur KulitDocument56 pagesBab 7. Struktur KulityumizoneNo ratings yet
- Bab 18 PsoriasisDocument53 pagesBab 18 PsoriasisyumizoneNo ratings yet
- Fitzpatrick Bab 154Document14 pagesFitzpatrick Bab 154yumizoneNo ratings yet
- Fitzpatrick Bab 155Document29 pagesFitzpatrick Bab 155yumizoneNo ratings yet
- Numata 2015Document2 pagesNumata 2015yumizoneNo ratings yet
- Brown 1987Document6 pagesBrown 1987yumizoneNo ratings yet
- Wolf 2001Document7 pagesWolf 2001yumizoneNo ratings yet
- Current Perspectives on Actinic Keratosis: A Review of Prevalence, Risk Factors, and Treatment OptionsDocument9 pagesCurrent Perspectives on Actinic Keratosis: A Review of Prevalence, Risk Factors, and Treatment OptionsyumizoneNo ratings yet
- Pendu Kung 1Document7 pagesPendu Kung 1yumizoneNo ratings yet
- Paget DiseaseDocument6 pagesPaget DiseaseyumizoneNo ratings yet
- Gynecologic Oncology: Hiroko Machida, Aida Moeini, Lynda D. Roman, Koji MatsuoDocument7 pagesGynecologic Oncology: Hiroko Machida, Aida Moeini, Lynda D. Roman, Koji MatsuoyumizoneNo ratings yet
- Febuxostat in GoutDocument7 pagesFebuxostat in GoutLia NadaNo ratings yet
- CBT NotesDocument8 pagesCBT NotesNom Nom75% (4)
- Endocrine CasesDocument12 pagesEndocrine Casesعلي. احمدNo ratings yet
- Clinical Clerkship Manual 2019 - 2020: University of Santo Tomas Faculty of Medicine and Surgery Clinical Programs OfficeDocument17 pagesClinical Clerkship Manual 2019 - 2020: University of Santo Tomas Faculty of Medicine and Surgery Clinical Programs OfficeJosh Jarold CoNo ratings yet
- Deshidratación Tipos Causas y Consecuencias - Rosa María OrtegaDocument2 pagesDeshidratación Tipos Causas y Consecuencias - Rosa María OrtegaJorge Cuadros CastroNo ratings yet
- National Institute of Indian Medical Heritage CatalogueDocument40 pagesNational Institute of Indian Medical Heritage CatalogueTapan Kumar MallickNo ratings yet
- Pre Feasibility Report of Pharmacy Business in PakistanDocument26 pagesPre Feasibility Report of Pharmacy Business in Pakistanzaheer100% (1)
- Laws Affecting Nursing Practice in the PhilippinesDocument6 pagesLaws Affecting Nursing Practice in the PhilippinesHuey Manalang Javier100% (1)
- Confusion: Koech KM Fri Feb 12, 2010Document23 pagesConfusion: Koech KM Fri Feb 12, 2010api-50425236No ratings yet
- Lecture-1-Introduction To Public HealthDocument24 pagesLecture-1-Introduction To Public HealthKaterina BagashviliNo ratings yet
- Webmm - Ahrq.gov.2 SlideshowDocument28 pagesWebmm - Ahrq.gov.2 SlideshowAlien_42No ratings yet
- Gambro AK 96® Dialysis Machine Operator's ManualDocument506 pagesGambro AK 96® Dialysis Machine Operator's ManualMahmoud Diaa90% (67)
- Fosfomycin-An Old-New AntibioticDocument4 pagesFosfomycin-An Old-New Antibioticvetma1No ratings yet
- Mode of Action of Abhyantara SnehanaDocument1 pageMode of Action of Abhyantara SnehananandkishorNo ratings yet
- Clinical Validation of A Test For The Diagnosis of VaginitisDocument9 pagesClinical Validation of A Test For The Diagnosis of Vaginitiserna utamiNo ratings yet
- ChemotherapyDocument11 pagesChemotherapyNedaAbdullahNo ratings yet
- tmp3741 TMPDocument8 pagestmp3741 TMPFrontiersNo ratings yet
- Defoer 1990Document8 pagesDefoer 1990Andreea CiorneaNo ratings yet
- Learning OverviewDocument18 pagesLearning Overviewsantosh mokasheNo ratings yet
- History of TriageDocument12 pagesHistory of Triageyuni purwatiNo ratings yet
- A Review of Inclusion Body Hepatitis-Hydropericardium Syndrome (Document24 pagesA Review of Inclusion Body Hepatitis-Hydropericardium Syndrome (Dr.Kedar Karki ,M.V.Sc.Preventive Vet.Medicine CLSU PhilippinesNo ratings yet
- Critical Thinking Case Study PharmaDocument4 pagesCritical Thinking Case Study PharmaChin T. OndongNo ratings yet
- Riluzole For SCZDocument11 pagesRiluzole For SCZHana Rizka AnandaNo ratings yet
- Mexico Market Regulatory Report2020Document22 pagesMexico Market Regulatory Report2020lindsayNo ratings yet
- 641 1769 1 PBDocument8 pages641 1769 1 PBHira DamayantiNo ratings yet
- PRC Form - orDocument5 pagesPRC Form - orJeaneline Pagasian EnonNo ratings yet
- Pain Dr. HenryDocument36 pagesPain Dr. Henryreagan setiawanNo ratings yet
- Mother Tinctures in HomoeopathyDocument9 pagesMother Tinctures in HomoeopathyRaghu ThotaNo ratings yet
- Types of Arrhythmias and Bradycardia Treatment AlgorithmsDocument18 pagesTypes of Arrhythmias and Bradycardia Treatment AlgorithmsZega AgustianNo ratings yet
- I. General Primary Health Care Facility Design Information: Research RequirementsDocument24 pagesI. General Primary Health Care Facility Design Information: Research RequirementsJoyce LapuzNo ratings yet