You might also like
- The Initial Prenatal Assessment and Routine Prenatal CareDocument16 pagesThe Initial Prenatal Assessment and Routine Prenatal Carelacminhhien100% (1)
- Lecture-28 Placenta PreviaDocument43 pagesLecture-28 Placenta PreviaMadhu Sudhan Pandeya100% (1)
- A. Menstrual Cycle Here Are Important Events During The Menstrual CycleDocument2 pagesA. Menstrual Cycle Here Are Important Events During The Menstrual CycleRosiro33% (3)
- Detailed Lesson Plan Science VDocument7 pagesDetailed Lesson Plan Science VAlizah Belle Garfin100% (1)
- Books For The Aspiring SexologistDocument2 pagesBooks For The Aspiring SexologistD HernandezNo ratings yet
- Animal Birth ControlDocument15 pagesAnimal Birth Controlvenku07484435No ratings yet
- Working During PregnancyDocument17 pagesWorking During Pregnancyjumgzb 10No ratings yet
- Chapter 5 - Letitia Richford - Cord ProlapseDocument6 pagesChapter 5 - Letitia Richford - Cord ProlapseEunice Cortés100% (1)
- Regular Exercise During Pregnancy To Prevent Gestational DiabetesDocument8 pagesRegular Exercise During Pregnancy To Prevent Gestational DiabetesEgie Nugraha Fitriyan ApriyadiNo ratings yet
- 2017 Article 632 PDFDocument11 pages2017 Article 632 PDFJauhiraNo ratings yet
- 2017 Article 1653Document11 pages2017 Article 1653amnatul khairiNo ratings yet
- Ffective For The Control of Gestational: Physical Activity Programs During Pregnancy Are E Diabetes MellitusDocument14 pagesFfective For The Control of Gestational: Physical Activity Programs During Pregnancy Are E Diabetes Mellitusellya nur safitriNo ratings yet
- 16-Full Paper (Without Author Information) - 102-1!4!20220302Document20 pages16-Full Paper (Without Author Information) - 102-1!4!20220302anjar ratihNo ratings yet
- PDF 3Document18 pagesPDF 3INA SAKTINo ratings yet
- Research Article: Age at Menarche, Menstrual Characteristics, and Risk of PreeclampsiaDocument6 pagesResearch Article: Age at Menarche, Menstrual Characteristics, and Risk of PreeclampsiaSyahrul Habibi NasutionNo ratings yet
- Effect of Socio-Demographic and Clinical Characteristics On Physical Activity of Pregnant Women at Referral Hospital in Riyadh, KSADocument7 pagesEffect of Socio-Demographic and Clinical Characteristics On Physical Activity of Pregnant Women at Referral Hospital in Riyadh, KSAArdika PutraNo ratings yet
- Pmed 1001036Document11 pagesPmed 1001036DorIta BojórquezNo ratings yet
- 08 AimukhametovaDocument10 pages08 AimukhametovahendraNo ratings yet
- Physical Activity and Dietary Habits During Pregnancy: Effects On Glucose ToleranceDocument6 pagesPhysical Activity and Dietary Habits During Pregnancy: Effects On Glucose ToleranceJulia ChuNo ratings yet
- BMJ f6398Document13 pagesBMJ f6398Luis Gerardo Pérez CastroNo ratings yet
- Journal Pone 0173937Document15 pagesJournal Pone 0173937Julenda CintarinovaNo ratings yet
- Bmi PregnancyDocument11 pagesBmi PregnancyLilik AnggrainiNo ratings yet
- Physical Activity Intensity and Type 2 Diabetes Risk in Overweight Youth A Randomized TriaDocument27 pagesPhysical Activity Intensity and Type 2 Diabetes Risk in Overweight Youth A Randomized TriaMilenckaVidalConsiglieriNo ratings yet
- A Cross-Sectional Survey of Australian Womens PerDocument43 pagesA Cross-Sectional Survey of Australian Womens PerMauricio CastroNo ratings yet
- Jurnal Referat 2Document7 pagesJurnal Referat 2nunki aprillitaNo ratings yet
- Clinical StudyDocument8 pagesClinical StudyanitaNo ratings yet
- Active Pregnancy Guide 2023Document65 pagesActive Pregnancy Guide 2023Nuno RobertoNo ratings yet
- Evaluation of A Smartphone Nutrition and Physical Activity Application To Provide Lifestyle Advice To Pregnant Women: The SNAPP Randomised TrialDocument11 pagesEvaluation of A Smartphone Nutrition and Physical Activity Application To Provide Lifestyle Advice To Pregnant Women: The SNAPP Randomised TrialTaís CidrãoNo ratings yet
- Ejercicio Funcion Vascular DiabetesDocument12 pagesEjercicio Funcion Vascular DiabetesMayra de CáceresNo ratings yet
- Pregnancy Exercise Overweight MetaanalysisDocument11 pagesPregnancy Exercise Overweight MetaanalysisAisleenHNo ratings yet
- Nutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsDocument15 pagesNutritional Prehabilitation Program and Cardiac Surgery Outcome in PediatricsIOSRjournalNo ratings yet
- The Influence of Smart Mother Classes Toward Stress, Childbirth Self-Efficacy and Birth OutcomesDocument9 pagesThe Influence of Smart Mother Classes Toward Stress, Childbirth Self-Efficacy and Birth OutcomesIJPHSNo ratings yet
- Postpartum Behaviour As Predictor of Weight Change From Before Pregnancy To One Year PostpartumDocument8 pagesPostpartum Behaviour As Predictor of Weight Change From Before Pregnancy To One Year PostpartumJm OpolintoNo ratings yet
- Research ArticleDocument6 pagesResearch ArticleRabiaNo ratings yet
- Or PD KehamilanDocument14 pagesOr PD KehamilanKurnia Fitri AprillianaNo ratings yet
- Research ArticleDocument8 pagesResearch Articlemohamad safiiNo ratings yet
- Jurnal Kesehatan MasyarakatDocument8 pagesJurnal Kesehatan MasyarakatDana AdwanNo ratings yet
- Effects of Structured Supervised Exercise Training or Motivational - Counseling On Pregnant Women's Physical Activity Level - FitMum - Randomized Controlled TrialDocument13 pagesEffects of Structured Supervised Exercise Training or Motivational - Counseling On Pregnant Women's Physical Activity Level - FitMum - Randomized Controlled TrialGabriela GutierrezNo ratings yet
- Currie2013 PDFDocument12 pagesCurrie2013 PDFheningdesykartikaNo ratings yet
- Patient Attitudes Toward Gestational Weight Gain and ExerciseDocument9 pagesPatient Attitudes Toward Gestational Weight Gain and ExercisealexNo ratings yet
- Senam Bugar Lansia Berpengaruh Terhadap Daya Tahan Jantung Paru, Status Gizi, Dan Tekanan DarahDocument9 pagesSenam Bugar Lansia Berpengaruh Terhadap Daya Tahan Jantung Paru, Status Gizi, Dan Tekanan DarahBilal MashelNo ratings yet
- Ijerph 17 02632 v2Document16 pagesIjerph 17 02632 v2Ricardo Martín MoyaNo ratings yet
- Jurnaal MaterDocument20 pagesJurnaal Materfebrin nocitaveraNo ratings yet
- M. Rizki Feiszal - 1706252Document9 pagesM. Rizki Feiszal - 1706252Rizqi ImdiansyahNo ratings yet
- Nutrition in Reproductive Health: Nutritional Conditioning Factors During Pregnancy and Its Impact On HealthDocument12 pagesNutrition in Reproductive Health: Nutritional Conditioning Factors During Pregnancy and Its Impact On HealthmamaazkaNo ratings yet
- Risk Factors of Pre-Eclampsia/Eclampsia and Its Adverse Outcomes in Low-And Middle-Income Countries: A WHO Secondary AnalysisDocument9 pagesRisk Factors of Pre-Eclampsia/Eclampsia and Its Adverse Outcomes in Low-And Middle-Income Countries: A WHO Secondary AnalysisPutri Nilam SariNo ratings yet
- Stener 2013Document8 pagesStener 2013Ke XuNo ratings yet
- Working During Pregnancy - UpToDateDocument20 pagesWorking During Pregnancy - UpToDatemariairenenoviNo ratings yet
- Jurnal Ibu Hamil Tidur PDFDocument9 pagesJurnal Ibu Hamil Tidur PDFBiyan TazqiyatusNo ratings yet
- Physical Activity, Body Mass Index, and Cardiorespiratory Fitness Among School Children in Taiwan: A Cross-Sectional StudyDocument11 pagesPhysical Activity, Body Mass Index, and Cardiorespiratory Fitness Among School Children in Taiwan: A Cross-Sectional StudyDurratulFajriPa'jioNo ratings yet
- ResearchDocument20 pagesResearchtedypsNo ratings yet
- Jurnal Novi 18 PDFDocument9 pagesJurnal Novi 18 PDFAndyk Strapilococus AureusNo ratings yet
- Jurnal Ibu MenopouseDocument15 pagesJurnal Ibu MenopouserahmatNo ratings yet
- BastaaDocument9 pagesBastaajohncarlo ramosNo ratings yet
- Evidence-Based Strategies For Managing Gestational Diabetes in Women With ObesityDocument11 pagesEvidence-Based Strategies For Managing Gestational Diabetes in Women With ObesityJasmine RoweNo ratings yet
- HolidaysDocument12 pagesHolidaysGabriela PopescuNo ratings yet
- Yong 2016Document8 pagesYong 2016yongyew2No ratings yet
- Jurnal RefreduksiDocument10 pagesJurnal RefreduksimusriahNo ratings yet
- Exercise and Sporting Activity During Pregnancy: Evidence-Based GuidelinesFrom EverandExercise and Sporting Activity During Pregnancy: Evidence-Based GuidelinesRita Santos-RochaNo ratings yet
- GDM, HapaDocument17 pagesGDM, HapaaisyarahmaNo ratings yet
- OGTT and Adverse Outcome 2020Document10 pagesOGTT and Adverse Outcome 2020Nuraida baharuddinNo ratings yet
- Evaluation of The 'Healthy Start To Pregnancy' Early Antenatal Health Promotion Workshop: A Randomized Controlled TrialDocument12 pagesEvaluation of The 'Healthy Start To Pregnancy' Early Antenatal Health Promotion Workshop: A Randomized Controlled TrialErfann Yuda AnsyariNo ratings yet
- Comparison of Serum Levels of Vitamin D and Inflammatory Markers Between Women With Gestational Diabetes Mellitus and Healthy Pregnant ControlDocument8 pagesComparison of Serum Levels of Vitamin D and Inflammatory Markers Between Women With Gestational Diabetes Mellitus and Healthy Pregnant ControlTaufik RizalNo ratings yet
- Bibliography Gestational DiabetesDocument3 pagesBibliography Gestational Diabetesregina.ann.gonsalvesNo ratings yet
- Metabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)Document15 pagesMetabolic Risk Management, Physical Exercise and Lifestyle Counselling in Low-Active Adults: Controlled Randomized Trial (BELLUGAT)adrianNo ratings yet
- Meta-Analysis The Effect of Obesity and Stress On Menstrual Cycle DisorderDocument13 pagesMeta-Analysis The Effect of Obesity and Stress On Menstrual Cycle DisorderMaria Angelika BughaoNo ratings yet
- Faal Partus: Naifah Luthfiyah Putri 15-009Document58 pagesFaal Partus: Naifah Luthfiyah Putri 15-009NaifahLuthfiyahPutriNo ratings yet
- During The PDocument15 pagesDuring The PApple Joy DiestroNo ratings yet
- NCM107 - Prelim - Teratogenic Maternal Infection and Psychological Changes in Pregnancy - Miss CabalangDocument7 pagesNCM107 - Prelim - Teratogenic Maternal Infection and Psychological Changes in Pregnancy - Miss CabalangLjc JaslinNo ratings yet
- Sigmund Freud'S Theory of Sexuality: Oral Stage (0-1 Year) : in The First Stage of Personality Development The Libido IsDocument2 pagesSigmund Freud'S Theory of Sexuality: Oral Stage (0-1 Year) : in The First Stage of Personality Development The Libido IsLudovica Dettin100% (1)
- Preparation For ParenthoodDocument2 pagesPreparation For Parenthoodtriniteacher77No ratings yet
- Episiotomi Repair Vicryl Rapide Vs VicrylDocument3 pagesEpisiotomi Repair Vicryl Rapide Vs VicrylamilyapraditaNo ratings yet
- EFMDocument15 pagesEFMslcNo ratings yet
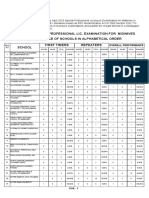
- April 2023 Special Professional Lic. Examination For MidwivesDocument2 pagesApril 2023 Special Professional Lic. Examination For MidwivesRapplerNo ratings yet
- Spontaneous and Re Ex OvulatorsDocument14 pagesSpontaneous and Re Ex OvulatorsFazal Akbar KhaliliNo ratings yet
- PatographDocument2 pagesPatographEvans Rogers NkanzaNo ratings yet
- Gynae Obs NuggetsDocument20 pagesGynae Obs Nuggetsdrusmansaleem100% (1)
- Period Poverty: Women Should Have Access To Free PadsDocument3 pagesPeriod Poverty: Women Should Have Access To Free Padsta bsNo ratings yet
- Gynae SNI Final Print VersionDocument34 pagesGynae SNI Final Print VersionMr Soman Nadim IqbalNo ratings yet
- Online Assignment 4Document15 pagesOnline Assignment 4Ab Staholic Boii100% (1)
- 983-Article Text-3702-1-10-20171114 PDFDocument10 pages983-Article Text-3702-1-10-20171114 PDFheni sulistya riniNo ratings yet
- Antepartum Fetal Surveillance ACOG Bulletin 2014 PDFDocument11 pagesAntepartum Fetal Surveillance ACOG Bulletin 2014 PDFDanNo ratings yet
- Ncam219 Lec PDFDocument102 pagesNcam219 Lec PDFDAVE BARIBENo ratings yet
- The Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousDocument8 pagesThe Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousNoraNo ratings yet
- FORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CareDocument2 pagesFORM 2E: Health Plan Implementation For: Maternal Health: Post-Partum CarePaul Mark PilarNo ratings yet
- Impact of Female Education On Fertility Perspective BangladeshDocument7 pagesImpact of Female Education On Fertility Perspective BangladeshBhudai123No ratings yet
- (Libro) The Role of Biotechnology in Improvement of Livestock Animal Health and Biotechnology-Muhammad Abubakar, Ali Saeed, ODocument151 pages(Libro) The Role of Biotechnology in Improvement of Livestock Animal Health and Biotechnology-Muhammad Abubakar, Ali Saeed, OramsesmuseNo ratings yet
- The High Risk New BornDocument23 pagesThe High Risk New Bornchhaiden100% (4)
- Pregnancy Induced HypertensionDocument21 pagesPregnancy Induced HypertensionLorren Frances Marie CalsarinNo ratings yet
- Maternal Health Nursing SkillsDocument279 pagesMaternal Health Nursing SkillsSharm ManlangitNo ratings yet