You might also like
- Epitome of the Pharmacopeia of the United States and the National Formulary: With CommentsFrom EverandEpitome of the Pharmacopeia of the United States and the National Formulary: With CommentsNo ratings yet
- Medicine To Buy in MexicoDocument3 pagesMedicine To Buy in MexicoJorgeErnestoMoncadaNo ratings yet
- ARTICAINE-articaine Hydrochloride and Epinephrine Injection, Solution Benco DentalDocument18 pagesARTICAINE-articaine Hydrochloride and Epinephrine Injection, Solution Benco DentalThu HiềnNo ratings yet
- Public Assessment Report for Helixor A Solution for InjectionDocument8 pagesPublic Assessment Report for Helixor A Solution for InjectionЈован Македонски ДулевNo ratings yet
- Statin Equipotent DosingDocument2 pagesStatin Equipotent DosingbencleeseNo ratings yet
- Lovenox InformationDocument80 pagesLovenox InformationWilliam RelucioNo ratings yet
- 2018 DPRI Booklet Nov-19-18Document23 pages2018 DPRI Booklet Nov-19-18Maria Lourdes MahusayNo ratings yet
- RIS2018 - For Pullout MedDocument156 pagesRIS2018 - For Pullout MedJZik SibalNo ratings yet
- Chemo Stability Chart LtoZDocument34 pagesChemo Stability Chart LtoZarfitaaaaNo ratings yet
- Cagayan Valley Medical Center: 2017 List of Procured and Consigned MedicinesDocument15 pagesCagayan Valley Medical Center: 2017 List of Procured and Consigned MedicinesJZik SibalNo ratings yet
- Cagayan Valley Medical Center: 2017 List of Procured and Consigned MedicinesDocument64 pagesCagayan Valley Medical Center: 2017 List of Procured and Consigned MedicinesAlex SibalNo ratings yet
- Business Profile of Genvio Pharma LimitedDocument5 pagesBusiness Profile of Genvio Pharma LimitedRashan Jida ReshanNo ratings yet
- Lovenox PDFDocument74 pagesLovenox PDFIntan Kusuma DewiNo ratings yet
- CatalogueDocument52 pagesCatalogueMeiliaty AngkyNo ratings yet
- Tripura Tender ProductsDocument2 pagesTripura Tender ProductsIntegrated user03No ratings yet
- B-Sitosterol HPLC UV JascoDocument4 pagesB-Sitosterol HPLC UV JascoAhmad AliNo ratings yet
- Analysis of Broad Spectrum' UVA and UVB Components in Sun Care Products For Compliance With New FDA RegulationsDocument2 pagesAnalysis of Broad Spectrum' UVA and UVB Components in Sun Care Products For Compliance With New FDA RegulationsMeral SüzerNo ratings yet
- Vial AmpDocument8 pagesVial AmpJacques DuriasNo ratings yet
- Binocrit Product Characteristics and Clinical UseDocument85 pagesBinocrit Product Characteristics and Clinical UseKhalil saterNo ratings yet
- CVMC Pharmacy Requisition and Issue Slip for Medications and SuppliesDocument154 pagesCVMC Pharmacy Requisition and Issue Slip for Medications and SuppliesAlex SibalNo ratings yet
- PH-PHR 315L Hospital Pharmacy First Semester AY 2020-2021 Module 5 Worksheet Pharmacy and Therapeutics Committee and Hospital Formulary SystemDocument15 pagesPH-PHR 315L Hospital Pharmacy First Semester AY 2020-2021 Module 5 Worksheet Pharmacy and Therapeutics Committee and Hospital Formulary SystemKyrie Gwynette OlarveNo ratings yet
- CORE LIST OF ESSENTIAL MEDICINESDocument13 pagesCORE LIST OF ESSENTIAL MEDICINESQueenee DalaloNo ratings yet
- Kit, Pneumonia, WHODocument2 pagesKit, Pneumonia, WHOEgas SaputraNo ratings yet
- Doh Do 0223Document19 pagesDoh Do 0223J Velasco PeraltaNo ratings yet
- District (Sadar) Hospital To A.P.H.C. Out Door: Essential Drug ListDocument5 pagesDistrict (Sadar) Hospital To A.P.H.C. Out Door: Essential Drug ListZiyaul Haq100% (1)
- Item 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16Document6 pagesItem 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16lipe167No ratings yet
- Ministry of Health Malaysia Drug Formulary NO. 3/2011Document31 pagesMinistry of Health Malaysia Drug Formulary NO. 3/2011Nina ShuibNo ratings yet
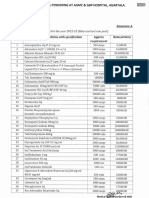
- Generic Name of Medicine (With Dosage Form and Strength) Brand Quantity Total Cost Supplier Manufacturer Acquisition CST Per UnitDocument72 pagesGeneric Name of Medicine (With Dosage Form and Strength) Brand Quantity Total Cost Supplier Manufacturer Acquisition CST Per UnitAlex SibalNo ratings yet
- Dpri 2016Document25 pagesDpri 2016Ferdinand Sta Ana Jr.No ratings yet
- Nitrile Gloves Cleared for Chemotherapy and Fentanyl UseDocument34 pagesNitrile Gloves Cleared for Chemotherapy and Fentanyl Usehitham shehataNo ratings yet
- MTLB - Group 3 FinalDocument9 pagesMTLB - Group 3 FinalRafael BrionesNo ratings yet
- Registration form for enzyme drugsDocument6 pagesRegistration form for enzyme drugsMd. Abdur RahmanNo ratings yet
- Fondaparinux Sodium Prefilled SyringeDocument19 pagesFondaparinux Sodium Prefilled SyringemeimanaloeNo ratings yet
- Dokumentacija ProcitajDocument44 pagesDokumentacija ProcitajNenad ŽivićNo ratings yet
- Summary Ubat 211 TambahanDocument31 pagesSummary Ubat 211 Tambahancks09No ratings yet
- Ua 702Document5 pagesUa 702hairiNo ratings yet
- MINISTRY OF HEALTH MALAYSIA DRUG FORMULARY UPDATEDocument31 pagesMINISTRY OF HEALTH MALAYSIA DRUG FORMULARY UPDATEweehanNo ratings yet
- DPRI 2016 Drug Price Reference IndexDocument25 pagesDPRI 2016 Drug Price Reference IndexBea del FierroNo ratings yet
- ES V 0281 001 FinalSPCDocument4 pagesES V 0281 001 FinalSPCPankaj BeniwalNo ratings yet
- Eprex LeafletDocument27 pagesEprex LeafletAbu MsrNo ratings yet
- (No. of Patients) (No. of Patients)Document4 pages(No. of Patients) (No. of Patients)Nav RNo ratings yet
- Furfural: EPA Pesticide Fact SheetDocument27 pagesFurfural: EPA Pesticide Fact SheetSteinerPDPNo ratings yet
- ChemoStabilityChartApril2013 Formatted 2Document90 pagesChemoStabilityChartApril2013 Formatted 2Fyana PutriNo ratings yet
- FT Artinibsa 40 MGML 0.01 MG ENDocument9 pagesFT Artinibsa 40 MGML 0.01 MG ENهشام موسىNo ratings yet
- Endotoxin LimitsDocument25 pagesEndotoxin LimitsAna AnitaNo ratings yet
- Pharmacokinetic and Pharmacodynamic AtorvastatinDocument23 pagesPharmacokinetic and Pharmacodynamic AtorvastatinEvitaIrmayantiNo ratings yet
- 2022 - July - 25 - Drug Price Reference IndexDocument45 pages2022 - July - 25 - Drug Price Reference Indexkhara teanoNo ratings yet
- Mycotoxin Reference and Research MaterialsDocument23 pagesMycotoxin Reference and Research MaterialsDana StoinNo ratings yet
- Central Pharmacy Stock Report Form: Action Contre La FaimDocument2 pagesCentral Pharmacy Stock Report Form: Action Contre La Faimmyatchitshin4121No ratings yet
- Calcium 2 - ADVIA Chemistry - Rev F DXDCM 09008b8380807ed3-1470363440603Document12 pagesCalcium 2 - ADVIA Chemistry - Rev F DXDCM 09008b8380807ed3-1470363440603mnemonicsNo ratings yet
- Essential List On 5th November 2022Document9 pagesEssential List On 5th November 2022AFI FARMANo ratings yet
- Reference For FDCDocument13 pagesReference For FDCJagdish ChanderNo ratings yet
- Draft Monograph For The International: PharmacopoeiaDocument6 pagesDraft Monograph For The International: PharmacopoeiaErnest Salazar Velazquez0% (1)
- PH Info ExamDocument44 pagesPH Info ExamANa AntonioNo ratings yet
- Drug CompilationDocument39 pagesDrug CompilationANa AntonioNo ratings yet
- Vanishree 1 PDFDocument1 pageVanishree 1 PDFKANTHA RAJUNo ratings yet
- Health Monitor USPADocument92 pagesHealth Monitor USPATorpe DonNo ratings yet
- 2018 DPRI Booklet FinalDocument20 pages2018 DPRI Booklet Finalkkabness101 YUL100% (1)
- Dimensional Analysis For Nursing StudentsFrom EverandDimensional Analysis For Nursing StudentsNo ratings yet
- Soleimani 2019Document5 pagesSoleimani 2019Chirac OanaNo ratings yet
- Martinez 2015Document1 pageMartinez 2015Chirac OanaNo ratings yet
- Temple 1981Document6 pagesTemple 1981Chirac OanaNo ratings yet
- Settipane 1981Document5 pagesSettipane 1981Chirac OanaNo ratings yet
- Dinakaran 2017Document16 pagesDinakaran 2017Chirac OanaNo ratings yet
- Guslandi 1997Document5 pagesGuslandi 1997Chirac OanaNo ratings yet
- Aspirin Therapy Risks and PreventionDocument19 pagesAspirin Therapy Risks and PreventionSaiful MukminNo ratings yet
- Decribing Places Buildings Successful Writing - Intermediate SBDocument6 pagesDecribing Places Buildings Successful Writing - Intermediate SBChirac OanaNo ratings yet
- WHOPIR BB NCIPD 11-13march2020Document15 pagesWHOPIR BB NCIPD 11-13march2020Chirac OanaNo ratings yet
- Hofbauer 2015Document5 pagesHofbauer 2015Chirac OanaNo ratings yet
- Combinatorial Test Design (CTD) : IBM Haifa Research LaboratoryDocument7 pagesCombinatorial Test Design (CTD) : IBM Haifa Research LaboratoryChirac OanaNo ratings yet
- ASCO Adjuvant Intravesical BCGDocument8 pagesASCO Adjuvant Intravesical BCGChirac OanaNo ratings yet
- Aspirin Dose and GI ToxicityDocument4 pagesAspirin Dose and GI ToxicityChirac OanaNo ratings yet
- Nacc Catalog - WebDocument54 pagesNacc Catalog - WebChirac OanaNo ratings yet
- LVD Directive 2014 - 35Document20 pagesLVD Directive 2014 - 35Raj PrasanthNo ratings yet
- Conflict of Interest Disclosures: Patient Case # 1Document28 pagesConflict of Interest Disclosures: Patient Case # 1Chirac OanaNo ratings yet
- Romanian Pharmacovigilance Workshop RegistrationDocument1 pageRomanian Pharmacovigilance Workshop RegistrationChirac OanaNo ratings yet
- Modularea Biochimica A Migrenei PDFDocument10 pagesModularea Biochimica A Migrenei PDFChirac OanaNo ratings yet
- Meropenem VenusDocument7 pagesMeropenem VenusChirac OanaNo ratings yet
- Modularea Biochimica A Migrenei PDFDocument10 pagesModularea Biochimica A Migrenei PDFChirac OanaNo ratings yet
- Year 9 - Speeding Up - Pressure and MomentsDocument10 pagesYear 9 - Speeding Up - Pressure and MomentsAmarpreet KaurNo ratings yet
- Microencapsulation Techniques and ApplicationsDocument17 pagesMicroencapsulation Techniques and ApplicationsHuma Hameed DogarNo ratings yet
- Artcles AP Kharif 05Document33 pagesArtcles AP Kharif 05api-3833893No ratings yet
- Triple Effect EvaporatorDocument9 pagesTriple Effect Evaporatorjnmanivannan100% (1)
- Convert I DoDocument43 pagesConvert I Do71403971No ratings yet
- Mechanical data sheet for diesel storage tankDocument2 pagesMechanical data sheet for diesel storage tankrifkynetNo ratings yet
- (Peter C. Foster) Easy Mathematics For Biologists PDFDocument114 pages(Peter C. Foster) Easy Mathematics For Biologists PDFSalsabila AnnisaNo ratings yet
- Z227caec6 - CC 102 - Module 7C - Solution - Dilution of SolutionDocument5 pagesZ227caec6 - CC 102 - Module 7C - Solution - Dilution of SolutionRona LucesNo ratings yet
- C72IA001EN-C Application Report ChitosanDocument4 pagesC72IA001EN-C Application Report ChitosanMartín PerezNo ratings yet
- Ion Exchange and Titration Detn Co and NiDocument6 pagesIon Exchange and Titration Detn Co and NiHoang ThaoNo ratings yet
- Safety Analysis Function Evaluation (S.A.F.E.) Chart: Project Document No. RevisionDocument19 pagesSafety Analysis Function Evaluation (S.A.F.E.) Chart: Project Document No. RevisionCandraNo ratings yet
- SG1 Final PPT Rev1Document51 pagesSG1 Final PPT Rev1Swarnim RajNo ratings yet
- Factors Affecting PharmacokineticsDocument9 pagesFactors Affecting PharmacokineticsLawrentian JadoonNo ratings yet
- Rhodia Sds Rhodacal 70-b CA z8Document17 pagesRhodia Sds Rhodacal 70-b CA z8Umair SuhailNo ratings yet
- QUIZ Confined Space Rescue AnswersDocument3 pagesQUIZ Confined Space Rescue AnswersEdwardNo ratings yet
- Animal Cell CultureDocument74 pagesAnimal Cell CultureMarcelo Andrés Ortiz BentoNo ratings yet
- The Feasibility Study of Calcium Phosphate Made - Docx, PR2Document22 pagesThe Feasibility Study of Calcium Phosphate Made - Docx, PR2diane camansagNo ratings yet
- Non Food ItemsDocument3 pagesNon Food ItemsAcfguam Acct IINo ratings yet
- Thermaline 4674: Selection & Specification DataDocument3 pagesThermaline 4674: Selection & Specification DataAlain AlexanderNo ratings yet
- Royal Botanic Gardens Victoria: Cranbourne Gardens Water Treatment PlantDocument40 pagesRoyal Botanic Gardens Victoria: Cranbourne Gardens Water Treatment PlantHenry OkoyeNo ratings yet
- Chemistry Investigatory Project On BrownDocument13 pagesChemistry Investigatory Project On BrownBRIJESH DWIVEDINo ratings yet
- Biogas Purification Using AmineDocument9 pagesBiogas Purification Using AmineAlbertIvanoAndreanNo ratings yet
- Acids and Bases PDFDocument25 pagesAcids and Bases PDFAnonymous Up4OeicsNo ratings yet
- PREP Hexanitrocobaltate(III) ionDocument3 pagesPREP Hexanitrocobaltate(III) ionSinenhlahla Thethwayo0% (1)
- Geochemical Analytical TechniquesDocument8 pagesGeochemical Analytical Techniquesapi-367976522No ratings yet
- Presentation by Mr. Amit Chaturvedi and Mr. Rajesh Rawat, Reliance IndustriesDocument18 pagesPresentation by Mr. Amit Chaturvedi and Mr. Rajesh Rawat, Reliance Industriesswaggeroni yololoNo ratings yet
- HW ID AmendmentDocument1 pageHW ID AmendmentZhu Chen ChuanNo ratings yet
- Hazard Communication Quiz-2: (B) DangerDocument3 pagesHazard Communication Quiz-2: (B) DangerJanak LalNo ratings yet
- The Liquid-Liquid Extraction of Toxic Metals (CD, HG and PB) by CalixarenesDocument13 pagesThe Liquid-Liquid Extraction of Toxic Metals (CD, HG and PB) by CalixarenesZaid A. AlalawiNo ratings yet