You might also like
- 16IJPHY343 C.doneDocument6 pages16IJPHY343 C.doneMiaNo ratings yet
- The Effect of Addition Kinesio Taping To Mckenzie Exercise in Patient With Chronic Mechanical Low Back PainDocument4 pagesThe Effect of Addition Kinesio Taping To Mckenzie Exercise in Patient With Chronic Mechanical Low Back PainRama BayuNo ratings yet
- Effects of Six-Week Exercise Training Protocol On Pain Relief in Patients With Lumbar Disc HerniationDocument7 pagesEffects of Six-Week Exercise Training Protocol On Pain Relief in Patients With Lumbar Disc HerniationAlexandra NistorNo ratings yet
- Manual Mobilization and EpicondylitisDocument11 pagesManual Mobilization and Epicondylitisterma83No ratings yet
- 8600Document8 pages8600elchinovichileno420No ratings yet
- Effect of NMES Vs Isometric Exercise in OA of Knee-With-Cover-Page-V2 Removed RemovedDocument5 pagesEffect of NMES Vs Isometric Exercise in OA of Knee-With-Cover-Page-V2 Removed RemovedZahra SativaniNo ratings yet
- An Adherent Nerve Root - Classification and Exercise Therapy in A PatientDocument4 pagesAn Adherent Nerve Root - Classification and Exercise Therapy in A PatientPablo Zamora MillanNo ratings yet
- Efficacy of Lumbar Mobilization On Postpartum Low Back Pain in Egyptian Females: A Randomized Control TrialDocument12 pagesEfficacy of Lumbar Mobilization On Postpartum Low Back Pain in Egyptian Females: A Randomized Control TrialAlekaNo ratings yet
- The Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyDocument5 pagesThe Effect of Spinal Exercises On H-Reflex in Subjects With Lumbosacral RadiculopathyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ughreja Myofascial ReleaseDocument9 pagesUghreja Myofascial Releasecris.endo.ceNo ratings yet
- Physiotherapy Management in Lumbar Facet Joint Syndrome - A Single Case StudyDocument5 pagesPhysiotherapy Management in Lumbar Facet Joint Syndrome - A Single Case StudyCambriaChicoNo ratings yet
- Piriformis Syndrome Treatment EffectivenessDocument5 pagesPiriformis Syndrome Treatment EffectivenessPraktek Fisioterapi Mitra SempajaNo ratings yet
- HVT With Lumbar Disc HerniationDocument12 pagesHVT With Lumbar Disc HerniationSheena McLennanNo ratings yet
- Background:: TH ST THDocument6 pagesBackground:: TH ST THRahayu WindariNo ratings yet
- تنزيلDocument7 pagesتنزيلDr Abdallah BahaaNo ratings yet
- MSK Pain LBPDocument12 pagesMSK Pain LBPMd. Ariful IslamNo ratings yet
- Lumbar StabilizationDocument16 pagesLumbar StabilizationSahithya MNo ratings yet
- Spinal Manipulation For Low-Back Pain: Key PointsDocument6 pagesSpinal Manipulation For Low-Back Pain: Key PointsInternational Business TimesNo ratings yet
- Treatment of Chronic Lower Back Pain With Lumbar Extension and Whole-Body Vibration ExerciseDocument6 pagesTreatment of Chronic Lower Back Pain With Lumbar Extension and Whole-Body Vibration ExerciseSuci NivlaharmyNo ratings yet
- American Osteopathic Association Guidelines For Osteopathic Manipulative TreatmentDocument14 pagesAmerican Osteopathic Association Guidelines For Osteopathic Manipulative TreatmentPaola GuerraNo ratings yet
- Does Moderate-To-High Intensity Nordic Walking Improve Functional Capacity and Pain in Fibromyalgia? A Prospective Randomized Controlled TrialDocument10 pagesDoes Moderate-To-High Intensity Nordic Walking Improve Functional Capacity and Pain in Fibromyalgia? A Prospective Randomized Controlled Trialrocio66No ratings yet
- Effect of Neural Mobilization Exercises in Patients With Low Back-Related Leg Pain With Peripheral Nerve Sensitization: A Prospective, Controlled TrialDocument11 pagesEffect of Neural Mobilization Exercises in Patients With Low Back-Related Leg Pain With Peripheral Nerve Sensitization: A Prospective, Controlled TrialJaniNo ratings yet
- Effectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFDocument5 pagesEffectiveness of Core Stabilization Exercises and Routine Exercise Therapy in Management of Pain in Chronic Non-Specific Low Back Pain A Randomized Controlled Clinical Trial PDFFelipe solis jimenez100% (1)
- Giray 2019Document13 pagesGiray 2019Felix LoaizaNo ratings yet
- The Evaluating of Efficacy of Mckenzie Exercises, Massage and Foot Reflexology On Pain and Disability of Men With Mechanical Chronic Low Back PainDocument7 pagesThe Evaluating of Efficacy of Mckenzie Exercises, Massage and Foot Reflexology On Pain and Disability of Men With Mechanical Chronic Low Back PainCarlos RiveraNo ratings yet
- 166-Article Text-300-1-10-20190603Document4 pages166-Article Text-300-1-10-20190603Achmad JunaidiNo ratings yet
- Effect of Isometric Quadriceps Exercise On Muscle StrengthDocument7 pagesEffect of Isometric Quadriceps Exercise On Muscle StrengthAyu RoseNo ratings yet
- Article 9Document8 pagesArticle 9umair muqriNo ratings yet
- Taise Angeli Boff, Fernanda Pasinato, Ângela Jornada Ben, Judith E. Bosmans, Maurits Van Tulder, Rodrigo Luiz CarregaroDocument10 pagesTaise Angeli Boff, Fernanda Pasinato, Ângela Jornada Ben, Judith E. Bosmans, Maurits Van Tulder, Rodrigo Luiz CarregaroNaomiNo ratings yet
- 24 - JPTS 2012 156Document4 pages24 - JPTS 2012 156Βιβιλάκη ΓεωργίαNo ratings yet
- JurnalDocument6 pagesJurnalAulia ElmaNo ratings yet
- Pi Is 000399931300453 XDocument7 pagesPi Is 000399931300453 XFarhaanKhanHaleemNo ratings yet
- ShareefDocument12 pagesShareefParaschiva PîțuNo ratings yet
- Moore 2013Document9 pagesMoore 2013Andrés MardonesNo ratings yet
- Effects of Repetitive Peripheral Magnetic Stimulation On Patients With Acute Low Back Pain: A Pilot StudyDocument10 pagesEffects of Repetitive Peripheral Magnetic Stimulation On Patients With Acute Low Back Pain: A Pilot StudyAnis AnwasNo ratings yet
- A Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder PatientsDocument4 pagesA Comparative Study To Determine The Efficacy of Routine Physical Therapy Treatment With and Without Kaltenborn Mobilization On Pain and Shoulder Mobility in Frozen Shoulder Patientsfi.afifah NurNo ratings yet
- Interventional Treatment For Myofascial Pelvic Floor...............Document10 pagesInterventional Treatment For Myofascial Pelvic Floor...............Andres MahechaNo ratings yet
- Maddalozzo 2018Document8 pagesMaddalozzo 2018Rolando TijerinaNo ratings yet
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchAritha HandricoNo ratings yet
- PNF Ombro 04Document10 pagesPNF Ombro 04Isaias AlmeidaNo ratings yet
- Article 4Document10 pagesArticle 4umair muqriNo ratings yet
- 2022 Article 3212Document15 pages2022 Article 3212LeidyNo ratings yet
- Effects of Thoracic Mobilization and Manipulation On Function and Mental State in Chronic Lower Back PainDocument4 pagesEffects of Thoracic Mobilization and Manipulation On Function and Mental State in Chronic Lower Back PainRatna Sulistya DewiNo ratings yet
- PNF Ombro 05Document19 pagesPNF Ombro 05Isaias AlmeidaNo ratings yet
- 10 1016@j Physio 2019 11 002Document27 pages10 1016@j Physio 2019 11 002Milton Ricardo de Medeiros FernandesNo ratings yet
- Hancock 2005Document6 pagesHancock 2005Elizabeth VivancoNo ratings yet
- A Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyDocument8 pagesA Structured Physiotherapy Treatment Model Can Provide Rapid Relief To Patients Who Qualify For Lumbar Disc Surgery: A Prospective Cohort StudyQuiroprácticaParaTodosNo ratings yet
- Conventional Therapy Versus Positional Release Technique in The Treatment of Chronic Low Back DysfunctionDocument7 pagesConventional Therapy Versus Positional Release Technique in The Treatment of Chronic Low Back DysfunctionEmad Eldin Mohamed AbdelatiefNo ratings yet
- Chronic Back PainDocument6 pagesChronic Back PaininnyNo ratings yet
- Journal ComparedDocument4 pagesJournal ComparedRisalah Al KhaerNo ratings yet
- Treating Lumbar SpondylosisDocument10 pagesTreating Lumbar SpondylosisDiyya Awaliah Nurhakiimah IbrahimNo ratings yet
- Pelvic Pain in Maigne's Syndrome-A Multi-Segmental ApproachDocument4 pagesPelvic Pain in Maigne's Syndrome-A Multi-Segmental Approachmanick.naguptNo ratings yet
- PQ Art 37583-10Document7 pagesPQ Art 37583-10Vinay KumarNo ratings yet
- Chronic Ankle InstabilityDocument9 pagesChronic Ankle InstabilityJonathan Elias Barrientos OssesNo ratings yet
- UntitledDocument7 pagesUntitledElizabeth VivancoNo ratings yet
- 2017 PNF and Manual Therapy Treatment Results of Cervical OADocument7 pages2017 PNF and Manual Therapy Treatment Results of Cervical OApainfree888100% (1)
- 7 Cochrane - UltrasoundGuided Percutaneous Electrolysis andDocument10 pages7 Cochrane - UltrasoundGuided Percutaneous Electrolysis andFranco Suazo MoralesNo ratings yet
- Efficacy of Pulsed Electromagnetic Therapy For Chronic Lower Back Pain: A Randomized, Double-Blind, Placebo-Controlled StudyDocument8 pagesEfficacy of Pulsed Electromagnetic Therapy For Chronic Lower Back Pain: A Randomized, Double-Blind, Placebo-Controlled StudyKyteNo ratings yet
- Acupressure For Chronic Low Back Pain: A Single System StudyDocument5 pagesAcupressure For Chronic Low Back Pain: A Single System StudyLelya Reema FitriaNo ratings yet
- Interventional Radiology of the Spine: Image-Guided Pain TherapyFrom EverandInterventional Radiology of the Spine: Image-Guided Pain TherapyJ. Kevin McGrawNo ratings yet
- Ulnar Nerve Injuries: Merugu Sahithya MPT OrthopaedicsDocument30 pagesUlnar Nerve Injuries: Merugu Sahithya MPT OrthopaedicsSahithya MNo ratings yet
- Art 1790040403 PDFDocument7 pagesArt 1790040403 PDFSahithya MNo ratings yet
- Achilles Tendinopathy CausesDocument7 pagesAchilles Tendinopathy CausesSahithya MNo ratings yet
- Art 1790040403 PDFDocument7 pagesArt 1790040403 PDFSahithya MNo ratings yet
- Musculoskeletal Disorders Part 5 Spinal Column DeformitiesDocument82 pagesMusculoskeletal Disorders Part 5 Spinal Column DeformitiesCarmela Lacsa Domocmat100% (1)
- Shoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesDocument3 pagesShoulder Pain in Hemiplegia: Statistical Relationship With Five VariablesSahithya MNo ratings yet
- The Source of Shoulder Pain in Hemiplegia: Robert L. Joynt, MDDocument5 pagesThe Source of Shoulder Pain in Hemiplegia: Robert L. Joynt, MDSahithya MNo ratings yet
- Coronal Alignment: After Total Knee ReplacementDocument6 pagesCoronal Alignment: After Total Knee ReplacementSahithya MNo ratings yet
- Does Total Knee Replacement Restore NormDocument9 pagesDoes Total Knee Replacement Restore NormSahithya MNo ratings yet
- Questionnaire On The Perceptions of Patients About Total Knee ReplacementDocument8 pagesQuestionnaire On The Perceptions of Patients About Total Knee ReplacementSahithya MNo ratings yet
- Alignment in Total Knee Replacement: Review ArticleDocument7 pagesAlignment in Total Knee Replacement: Review ArticleSahithya MNo ratings yet
- Edinburgh Research Explorer: Predicting Dissatisfaction Following Total Knee ReplacementDocument7 pagesEdinburgh Research Explorer: Predicting Dissatisfaction Following Total Knee ReplacementSahithya MNo ratings yet
- Shoulder Pain in Wheelchair Users With Tetraplegia and ParaplegiaDocument5 pagesShoulder Pain in Wheelchair Users With Tetraplegia and ParaplegiaSahithya MNo ratings yet
- Patient Outcomes Following Tricompartmental Total Knee Replacement: A Meta-AnalysisDocument3 pagesPatient Outcomes Following Tricompartmental Total Knee Replacement: A Meta-AnalysisSahithya MNo ratings yet
- BLR TechniqueDocument5 pagesBLR TechniqueDeva JCNo ratings yet
- Physio Rehab TKRDocument91 pagesPhysio Rehab TKRSahithya MNo ratings yet
- Infection As A Complication of Total Knee-Replacement ArthroplastyDocument6 pagesInfection As A Complication of Total Knee-Replacement ArthroplastySahithya MNo ratings yet
- (92 99) V9N6PT PDFDocument8 pages(92 99) V9N6PT PDFBoobesh Venkata RamananNo ratings yet
- Mets and Core StabilityDocument8 pagesMets and Core StabilitySahithya MNo ratings yet
- Ortho Manual Therapy, MckenzieDocument6 pagesOrtho Manual Therapy, MckenzieSahithya MNo ratings yet
- MFR With Core StabilityDocument12 pagesMFR With Core StabilitySahithya MNo ratings yet
- Mechanical Factors and Incidence of LbaDocument20 pagesMechanical Factors and Incidence of LbaSahithya MNo ratings yet
- Manual Therapy Followed by Specific Active ExercisesDocument11 pagesManual Therapy Followed by Specific Active ExercisesSahithya MNo ratings yet
- Effects of Maitland Mobilization and Mul PDFDocument6 pagesEffects of Maitland Mobilization and Mul PDFKuroha Hagane KunNo ratings yet
- Maitland Vs ShaclocksDocument1 pageMaitland Vs ShaclocksSahithya MNo ratings yet
- Aure 2003Document8 pagesAure 2003Charlotte WilliamsNo ratings yet
- Physiotherapy: P. Ratan Khuman Lourembam Surbala Priyanka Patel Dhara ChavdaDocument4 pagesPhysiotherapy: P. Ratan Khuman Lourembam Surbala Priyanka Patel Dhara ChavdaSahithya MNo ratings yet
- Maitland Vs Mckenzie With Core StbaltyDocument71 pagesMaitland Vs Mckenzie With Core StbaltySahithya MNo ratings yet
- Effects of Maitland Mobilization and Mul PDFDocument6 pagesEffects of Maitland Mobilization and Mul PDFKuroha Hagane KunNo ratings yet
- Maitland Vs Mckenzie Press UpDocument309 pagesMaitland Vs Mckenzie Press UpSahithya M100% (1)
- OD2e L3 Tests Skills Test 1Document4 pagesOD2e L3 Tests Skills Test 1Elo CáceresNo ratings yet
- Positioning Getting Open Without The BallDocument8 pagesPositioning Getting Open Without The BallAlexNo ratings yet
- Gazette A 2009-IIIDocument500 pagesGazette A 2009-IIIarslanjamil_jamilNo ratings yet
- Bogie ShopDocument6 pagesBogie ShopPrasanna VermaNo ratings yet
- Fortnite Skin Generator - Generate A Set of Fortnite SkinsDocument2 pagesFortnite Skin Generator - Generate A Set of Fortnite SkinsKiirvss Ong0% (1)
- Red Dead Redemption Sheet Music Piano Bar Song PDFDocument2 pagesRed Dead Redemption Sheet Music Piano Bar Song PDFPierre RodriguezNo ratings yet
- IB MATH PORTFOLIO 1 - Infinite SummationDocument27 pagesIB MATH PORTFOLIO 1 - Infinite Summationmykiri790% (1)
- Golden Heroes RPGDocument3 pagesGolden Heroes RPGEric50% (2)
- Jsa - Cable Termination: Job Step No. Step Description Hazards Control Measure(s) Responsible PersonDocument7 pagesJsa - Cable Termination: Job Step No. Step Description Hazards Control Measure(s) Responsible PersonMon Trang NguyễnNo ratings yet
- ScorpioDocument2 pagesScorpioAmrit PrasadNo ratings yet
- Complete Wide Receiver PDFDocument305 pagesComplete Wide Receiver PDFmax100% (3)
- League of Legends Macro GuideDocument3 pagesLeague of Legends Macro Guidevolwer02100No ratings yet
- RoguePlanet Derelict Edition MasterDocument72 pagesRoguePlanet Derelict Edition MasterJulien Blin50% (2)
- 2019.04 Stringing Catalogue CDTDocument1 page2019.04 Stringing Catalogue CDTZlatanNo ratings yet
- Three Little PigsDocument29 pagesThree Little PigsSalman Valerio Delfin100% (1)
- Manual TransmisionDocument70 pagesManual TransmisionJose Figueroa100% (1)
- Carl de Crée - Kodokan Judo's Three Orphaned Forms of Countertechniques. Part 2. The Nage Waza Ura No Kata PDFDocument30 pagesCarl de Crée - Kodokan Judo's Three Orphaned Forms of Countertechniques. Part 2. The Nage Waza Ura No Kata PDFEdinson Valery EspinozaNo ratings yet
- Beginners Guide CrossFitDocument5 pagesBeginners Guide CrossFitAdam 'Buddha' McGrath100% (2)
- 150 Office/Tech:: Rifle IndexDocument42 pages150 Office/Tech:: Rifle IndexStan BrittsanNo ratings yet
- Da Annex10-04-19Document10 pagesDa Annex10-04-19Some GuyNo ratings yet
- Rezultate Inițiale Titularizare 2022Document20 pagesRezultate Inițiale Titularizare 2022Anca Iulia DișteanuNo ratings yet
- Copia de Inventario 25 Nov 22Document91 pagesCopia de Inventario 25 Nov 22Gretel Maite Mendoza PulidoNo ratings yet
- Front Suspension Section GuideDocument19 pagesFront Suspension Section GuideMrihexNo ratings yet
- Drill Manual Codes For SchedulesDocument89 pagesDrill Manual Codes For SchedulesBruno Oliveira Do NascimentoNo ratings yet
- WMKK PDFDocument78 pagesWMKK PDFJustin OngNo ratings yet
- 2011 WPFG Results New YorkDocument95 pages2011 WPFG Results New YorkForum PompieriiNo ratings yet
- Fuse Box Passat b6Document19 pagesFuse Box Passat b6Ionut AlbuicaNo ratings yet
- Sasot Vs PeopleDocument13 pagesSasot Vs PeopleUnsolicited CommentNo ratings yet
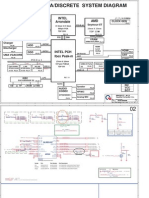
- HP Pavilion G4 G6 G7 Quanta R12 Rev 1A SCHDocument39 pagesHP Pavilion G4 G6 G7 Quanta R12 Rev 1A SCHZsootiNo ratings yet
- Manual de Despiece Cruiser 250Document43 pagesManual de Despiece Cruiser 250leanroy1130% (1)