You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Electrolyte Mnemonic QuizletDocument3 pagesElectrolyte Mnemonic QuizletA.h.Murad100% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hospital "Crash Cart" - MICU: Yatska Cartagena Juan MoralesDocument47 pagesHospital "Crash Cart" - MICU: Yatska Cartagena Juan Moralesmoralesjuan9100% (1)
- Path Endocrine OutlineDocument46 pagesPath Endocrine Outlineaya derweshNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Drug StudyDocument5 pagesDrug StudyAshley Jane MacapayadNo ratings yet
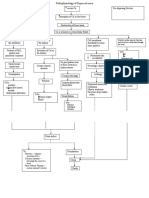
- Pathophysiology of HypercalcemiaDocument3 pagesPathophysiology of Hypercalcemiajoys11No ratings yet
- Parathyroid (Hyper & Hypo)Document1 pageParathyroid (Hyper & Hypo)Vishal100% (1)
- 10 EndocrinologyDocument223 pages10 Endocrinologythisar100% (1)
- Early Goal-Directed Therapy in The Treatment of Severe Sepsis and Septic ShockDocument10 pagesEarly Goal-Directed Therapy in The Treatment of Severe Sepsis and Septic ShockRetno SuminarNo ratings yet
- Proning in ARDSDocument10 pagesProning in ARDSAndrew DavidsonNo ratings yet
- Permissive Under Feeding AJRCCMDocument31 pagesPermissive Under Feeding AJRCCMcsquizzardNo ratings yet
- Permissive Underfeeding or Standard Enteral Feeding in Critically Ill AdultsDocument11 pagesPermissive Underfeeding or Standard Enteral Feeding in Critically Ill AdultsimNo ratings yet
- Vignon Echo Fluid ResponsivenessDocument46 pagesVignon Echo Fluid ResponsivenesscsquizzardNo ratings yet
- Stitch TrialDocument26 pagesStitch TrialcsquizzardNo ratings yet
- EWD340Document17 pagesEWD340computingdocs222No ratings yet
- 5 Minute Biochemistry PresentationDocument23 pages5 Minute Biochemistry PresentationPITAGAN, Galda Boy 1-FNo ratings yet
- Hemostan, Methergine CA Gluconate2Document4 pagesHemostan, Methergine CA Gluconate2Stacy MC PelitoNo ratings yet
- Zoledronic Acid Is Superior To Pamidronate in The Treatment of Hypercalcemia of Malignancy: A Pooled Analysis of Two Randomized, Controlled Clinical Trials - PubMedDocument2 pagesZoledronic Acid Is Superior To Pamidronate in The Treatment of Hypercalcemia of Malignancy: A Pooled Analysis of Two Randomized, Controlled Clinical Trials - PubMedMikeNo ratings yet
- Acid-Base Disorders Fluid and ElectrolytesDocument13 pagesAcid-Base Disorders Fluid and ElectrolytesNicole BiduaNo ratings yet
- Lecture Notes in Medical Technology - Lecture #6 - The PARATHYROID GLANDDocument15 pagesLecture Notes in Medical Technology - Lecture #6 - The PARATHYROID GLANDKat JornadalNo ratings yet
- Endocrine Physiology - Part 3 Parathyroid GlandDocument30 pagesEndocrine Physiology - Part 3 Parathyroid GlandTerrence Beniasi CharumbiraNo ratings yet
- Parathyroid DisordersDocument44 pagesParathyroid DisordersBIAN ALKHAZMARINo ratings yet
- Diagnosis and Management of HypocalcemiaDocument11 pagesDiagnosis and Management of HypocalcemiamdmmmNo ratings yet
- ESRDDocument46 pagesESRDquina mjNo ratings yet
- Ma A LoxDocument2 pagesMa A LoxMicah_Ela_Lao_2724No ratings yet
- Compound Sodium LactateDocument10 pagesCompound Sodium LactateershahasanNo ratings yet
- SC2 Sample Written Paper Questions With Answers 1Document11 pagesSC2 Sample Written Paper Questions With Answers 1Zi SongNo ratings yet
- 16-K-Ca ImbalanceDocument11 pages16-K-Ca Imbalanceمصطفى محمد جواد كاظمNo ratings yet
- Fluid TherapyDocument9 pagesFluid TherapyMadiha MadiNo ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- Symptoms of Paget S DiseaseDocument49 pagesSymptoms of Paget S DiseaseurufahoNo ratings yet
- National NORCET Prelims Test-1Document43 pagesNational NORCET Prelims Test-1SHIVANIINo ratings yet
- NCP Calcium ImbalanceDocument4 pagesNCP Calcium ImbalanceHazel MarananNo ratings yet
- Fluids and ElectrolytesDocument102 pagesFluids and Electrolytesfelxhu50% (2)
- Calcium GluconateDocument1 pageCalcium GluconateMary Reigns BuhatNo ratings yet
- Hiperparatiroidism SarcinaDocument7 pagesHiperparatiroidism SarcinaClaudia IrimieNo ratings yet
- Parathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismDocument25 pagesParathyroid Gland Diseases: Primary Hyperparathyroidism HypoparathyroidismZahrah El FaradisaNo ratings yet
- Hypercalcemia: Case StudyDocument11 pagesHypercalcemia: Case StudyMayka JacintoNo ratings yet