You might also like
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Parental Care and The Development of The Parent Offspring Conflict in Discus Fish (Symphysodon SPP.)Document298 pagesParental Care and The Development of The Parent Offspring Conflict in Discus Fish (Symphysodon SPP.)Ethan AmalNo ratings yet
- Anomalous Pulmonary Venous Connections and Related Anomalies - Nomenclature, Embryology, Anatomy, and MorphologyDocument16 pagesAnomalous Pulmonary Venous Connections and Related Anomalies - Nomenclature, Embryology, Anatomy, and MorphologyEthan AmalNo ratings yet
- Working Training NHS Guide For IMGsDocument26 pagesWorking Training NHS Guide For IMGsandreeamandoiuNo ratings yet
- Invitation and Agenda - Best in Class MV Repair 0829Document1 pageInvitation and Agenda - Best in Class MV Repair 0829Ethan AmalNo ratings yet
- Understanding The Morphology of The Specialized Conduction Tissues in Congenitally Malformed HeartsDocument11 pagesUnderstanding The Morphology of The Specialized Conduction Tissues in Congenitally Malformed HeartsEthan AmalNo ratings yet
- Working Training NHS Guide For IMGsDocument26 pagesWorking Training NHS Guide For IMGsandreeamandoiuNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument35 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEthan AmalNo ratings yet
- AA Issue-Article 9Document11 pagesAA Issue-Article 9Ethan AmalNo ratings yet
- Description of The Reproductive Behavior Of: Symphysodon Aequifasciatus (Cichlidae) in CaptivityDocument6 pagesDescription of The Reproductive Behavior Of: Symphysodon Aequifasciatus (Cichlidae) in CaptivityAranditza HernandezNo ratings yet
- Safety of Temporary Pacemaker WiresDocument20 pagesSafety of Temporary Pacemaker WiresEthan AmalNo ratings yet
- State of The Art Concepts in Aortic Valve Replacement: Please Join Us For The 90 MinutesDocument1 pageState of The Art Concepts in Aortic Valve Replacement: Please Join Us For The 90 MinutesEthan AmalNo ratings yet
- Edwards iBAR Agenda 16thoct ThailandDocument1 pageEdwards iBAR Agenda 16thoct ThailandEthan AmalNo ratings yet
- Anomalous Pulmonary Venous Connections and Related Anomalies - Nomenclature, Embryology, Anatomy, and MorphologyDocument16 pagesAnomalous Pulmonary Venous Connections and Related Anomalies - Nomenclature, Embryology, Anatomy, and MorphologyEthan AmalNo ratings yet
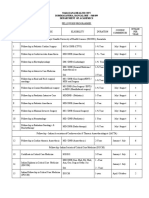
- Narayana Health City Bommasandra, Bangalore - 560 099 Department of AcademicsDocument2 pagesNarayana Health City Bommasandra, Bangalore - 560 099 Department of AcademicsEthan AmalNo ratings yet
- AA Issue-Article 9Document11 pagesAA Issue-Article 9Ethan AmalNo ratings yet
- Page Proof Instructions and Queries: Asian Cardiovascular & Thoracic Annals (AAN) 984097Document6 pagesPage Proof Instructions and Queries: Asian Cardiovascular & Thoracic Annals (AAN) 984097Ethan AmalNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument35 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsEthan AmalNo ratings yet
- Bps in Pediatric CentreDocument6 pagesBps in Pediatric CentreEthan AmalNo ratings yet
- Bps in Pediatric CentreDocument6 pagesBps in Pediatric CentreEthan AmalNo ratings yet
- Aortotomy and Endarterectomy of The Ascending Aorta For Aortic Valve Replacement in A Patient With Porcelain AortaDocument4 pagesAortotomy and Endarterectomy of The Ascending Aorta For Aortic Valve Replacement in A Patient With Porcelain AortaEthan AmalNo ratings yet
- An Analysis On The Use of Warren's Distal Splenorenal Shunt Surgery For The Treatment of Portal Hypertension at The University Hospitals Leuven PDFDocument8 pagesAn Analysis On The Use of Warren's Distal Splenorenal Shunt Surgery For The Treatment of Portal Hypertension at The University Hospitals Leuven PDFEthan AmalNo ratings yet
- Jurnal Reading Thorax BPSDocument15 pagesJurnal Reading Thorax BPSEthan AmalNo ratings yet
- Adenoca From SequestrationDocument4 pagesAdenoca From SequestrationEthan AmalNo ratings yet
- Example Asian AnnalsDocument6 pagesExample Asian AnnalsEthan AmalNo ratings yet
- Surgical Treatment of PAVMDocument5 pagesSurgical Treatment of PAVMEthan AmalNo ratings yet
- Surgical Repair of Stenotic Pulmonary Arteries in Tetralogy of FalllotDocument25 pagesSurgical Repair of Stenotic Pulmonary Arteries in Tetralogy of FalllotEthan AmalNo ratings yet
- Cardiac Arrhytmia During CVCDocument6 pagesCardiac Arrhytmia During CVCEthan AmalNo ratings yet
- Lobectomy in CcamDocument5 pagesLobectomy in CcamEthan AmalNo ratings yet
- Ccam N Bps Management PDFDocument9 pagesCcam N Bps Management PDFEthan AmalNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Studi Kasus Kegagalan Pada HatiDocument34 pagesStudi Kasus Kegagalan Pada HatiMarLeniRN100% (1)
- Educational Pre-Testing (KROK-2) : Quiz NavigationDocument1 pageEducational Pre-Testing (KROK-2) : Quiz NavigationMohammad MohyeddienNo ratings yet
- Lesson Plan On Post Natal ExercisesDocument11 pagesLesson Plan On Post Natal ExercisesRaja67% (6)
- Hatha Yoga BandhasDocument69 pagesHatha Yoga Bandhaspatil_goaNo ratings yet
- Ultrasonography of Pylorospasm: Findings May Simulate Hypertrophic Pyloric StenosisDocument7 pagesUltrasonography of Pylorospasm: Findings May Simulate Hypertrophic Pyloric StenosisGladysIndikaNo ratings yet
- Trace of Oxygen from Nose to Lungs to BodyDocument3 pagesTrace of Oxygen from Nose to Lungs to Bodyaznknight323No ratings yet
- Diccionario Esperanto - Inglés PDFDocument500 pagesDiccionario Esperanto - Inglés PDFDiego EmeNo ratings yet
- Frenchenglishmed00gorduoft BWDocument178 pagesFrenchenglishmed00gorduoft BWBranko NikolicNo ratings yet
- Idcases: Case ReportDocument3 pagesIdcases: Case ReportPeko PekoNo ratings yet
- Case Report: Urachal Adenocarcinoma: A Case Report With Key Imaging Findings and Radiologic-Pathologic CorrelationDocument6 pagesCase Report: Urachal Adenocarcinoma: A Case Report With Key Imaging Findings and Radiologic-Pathologic Correlationchristian hansNo ratings yet
- Interpretation of FibroScanDocument16 pagesInterpretation of FibroScanAAMIRNo ratings yet
- Ascad Asit For AnimalsDocument87 pagesAscad Asit For AnimalsThamil Arasan100% (1)
- CH 2 - Maternal AnatomyDocument8 pagesCH 2 - Maternal AnatomyRandom CommenterNo ratings yet
- ABDOMEN ANATOMY L Johari MBBSDocument99 pagesABDOMEN ANATOMY L Johari MBBSnimbudanimbuda1No ratings yet
- Diseases of The AbomasumDocument25 pagesDiseases of The AbomasumasddafadNo ratings yet
- (Fitness Sutra Book 1) Chopra, Dr. Monika - Workout For Desk Bounds - Quick Stretches & Exercises To Keep Your Neck, Shoulders, Back & Legs Pain-Free and Mind Active-Fitsutra Wellness PVT LTD (2020)Document138 pages(Fitness Sutra Book 1) Chopra, Dr. Monika - Workout For Desk Bounds - Quick Stretches & Exercises To Keep Your Neck, Shoulders, Back & Legs Pain-Free and Mind Active-Fitsutra Wellness PVT LTD (2020)Anh Le100% (2)
- DebnathExercise Plan 2 STR - Training - 17th Dec 2021Document3 pagesDebnathExercise Plan 2 STR - Training - 17th Dec 2021Amruta BhagwatNo ratings yet
- Belly-Cultivation Techniques as Healing Practices in Early 20th Century JapanDocument25 pagesBelly-Cultivation Techniques as Healing Practices in Early 20th Century JapanjsjsjjsNo ratings yet
- Yoga & Lifestyle: Topics of Unit: 3Document14 pagesYoga & Lifestyle: Topics of Unit: 3UNKNOWN KNOWLEDGENo ratings yet
- Abdominal Pain in AdultsDocument3 pagesAbdominal Pain in Adultshikmah_fajriantiNo ratings yet
- 10 BiologyDocument5 pages10 BiologyLegend 77 FFNo ratings yet
- 001 Abdominal Wall PathologyDocument285 pages001 Abdominal Wall PathologyKlari GabosNo ratings yet
- Lesson Plan in Science 4 - LajieDocument10 pagesLesson Plan in Science 4 - LajieMar JenNo ratings yet
- პანკრეასიDocument24 pagesპანკრეასიSASIDHARNo ratings yet
- What Are Gallstones?: Lemuel Jay A. Segovia Grade 8-Peace Science Q4M1Document4 pagesWhat Are Gallstones?: Lemuel Jay A. Segovia Grade 8-Peace Science Q4M1Zarah Joyce SegoviaNo ratings yet
- Abdomen - FRCEM SuccessDocument275 pagesAbdomen - FRCEM SuccessAbin ThomasNo ratings yet
- A 27-Year-Old Woman Presented With Three-Day History of Generalized Mild Abdominal PainDocument144 pagesA 27-Year-Old Woman Presented With Three-Day History of Generalized Mild Abdominal PainAldredNo ratings yet
- Energy Medicine Tips ChartDocument3 pagesEnergy Medicine Tips ChartAnastasia Haralambidou100% (9)
- Urinary SystemDocument20 pagesUrinary SystemKelvin MallariNo ratings yet
- Hepatobiliary SystemDocument2 pagesHepatobiliary SystemDarren J Menchavez LimaNo ratings yet