You might also like
- Osteosarcoma PDFDocument3 pagesOsteosarcoma PDFkc andrea torresNo ratings yet
- Cancer Nursing: By: Mrs. Theresa Margarita Marivee L. SaldevarDocument24 pagesCancer Nursing: By: Mrs. Theresa Margarita Marivee L. Saldevarfaithfabulous1_06100% (2)
- Additional Notes in Pedia Neuro2Document4 pagesAdditional Notes in Pedia Neuro2Geraldine Marie SalvoNo ratings yet
- A.K12 - FINAL Management Brain Tumors Dr. Dr. Rr. Suzy Indharty, M. Kes, SP - BsDocument42 pagesA.K12 - FINAL Management Brain Tumors Dr. Dr. Rr. Suzy Indharty, M. Kes, SP - BsandrianyNo ratings yet
- Bone Tumor Seminar: Types & ManagementDocument80 pagesBone Tumor Seminar: Types & ManagementPATHMAPRIYA GANESANNo ratings yet
- Skull Base Tumors Classification and ManagementDocument20 pagesSkull Base Tumors Classification and ManagementWinda HaeriyokoNo ratings yet
- Intradural, Extramedullary Spinal Tumors: BackgroundDocument9 pagesIntradural, Extramedullary Spinal Tumors: Backgroundmetasoniko81No ratings yet
- SARCOMA Bimbingan KoasDocument41 pagesSARCOMA Bimbingan KoasWarung MamakNo ratings yet
- Brain TumorDocument1 pageBrain TumorChase XerolfNo ratings yet
- NeuroblastomaDocument33 pagesNeuroblastomahariNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- Intradural Extramedullary TumorsDocument10 pagesIntradural Extramedullary TumorsFaizyab AhmedNo ratings yet
- SNP Envolvimento em Doentes Com Neoplasia Lancet 2007Document12 pagesSNP Envolvimento em Doentes Com Neoplasia Lancet 2007Gonçalo CabralNo ratings yet
- Radiation Therapy Treatment Planning and Post-Care GuideDocument93 pagesRadiation Therapy Treatment Planning and Post-Care GuideVyomaNo ratings yet
- Dermatology - Skin NeoplasmsDocument12 pagesDermatology - Skin NeoplasmsIsabel CastilloNo ratings yet
- 5 4b Childhood Malignancy Part 2 DR Melanie Victoria G DarDocument7 pages5 4b Childhood Malignancy Part 2 DR Melanie Victoria G DarSamatha SamathaNo ratings yet
- 2022 Article 10218Document9 pages2022 Article 10218Dinda SaviraNo ratings yet
- EPOSTER PABI Dr. Defri HeryadiDocument1 pageEPOSTER PABI Dr. Defri HeryadiSeptia Pristi RahmahNo ratings yet
- Applying Immune Checkpoint Inhibitor Therapy in The Clinical Management of SCLCDocument67 pagesApplying Immune Checkpoint Inhibitor Therapy in The Clinical Management of SCLCYasar HammorNo ratings yet
- Journal Reading Multiple Myeloma 1Document29 pagesJournal Reading Multiple Myeloma 1AristynrNo ratings yet
- Tumors of Musculoskeletal: Tutorial Ortopaedic SurgeryDocument108 pagesTumors of Musculoskeletal: Tutorial Ortopaedic SurgeryfarisNo ratings yet
- 2 - Spinal CordDocument32 pages2 - Spinal CordAsma AliNo ratings yet
- Types of Cancer Risk Factors Screenings TreatmentsDocument4 pagesTypes of Cancer Risk Factors Screenings TreatmentsEffie Cloe Marie BitengNo ratings yet
- Didactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Document28 pagesDidactics 3 - Neoplastic Diseases of The Salivary Glands (Autosaved)Moritz SolivenNo ratings yet
- (10920684 - Neurosurgical Focus) Intramedullary Spinal Cord Tumors - A Review of Current and Future Treatment StrategiesDocument10 pages(10920684 - Neurosurgical Focus) Intramedullary Spinal Cord Tumors - A Review of Current and Future Treatment StrategiesSachin RajaNo ratings yet
- Tumor MarkerDocument4 pagesTumor Markerkimmynemil80No ratings yet
- Adult Brainstem Gliomas ReviewDocument11 pagesAdult Brainstem Gliomas ReviewJuan Diego Martinez LemusNo ratings yet
- 72 - Skin CancerDocument1 page72 - Skin CancerRica Alyssa PepitoNo ratings yet
- Oral Pathology Dent1411Document7 pagesOral Pathology Dent1411api-663458841No ratings yet
- Kegawatan Respirasi Pada Keganasan Rongga ToraksDocument57 pagesKegawatan Respirasi Pada Keganasan Rongga ToraksChristian HarnatNo ratings yet
- Journal Review Orbital TumourDocument26 pagesJournal Review Orbital TumourbhartiNo ratings yet
- Metastaticeurospine2015 151207184233 Lva1 App6891Document122 pagesMetastaticeurospine2015 151207184233 Lva1 App6891niluhputu asrinidewiNo ratings yet
- Ewing SarcomaDocument2 pagesEwing SarcomaWilliam TanNo ratings yet
- Neoplasm of Musculoskeletal Tissue: A GuideDocument48 pagesNeoplasm of Musculoskeletal Tissue: A Guidehello from the other sideNo ratings yet
- DR - Ign Purna Putra, Sps (K)Document64 pagesDR - Ign Purna Putra, Sps (K)Sheryl ElitaNo ratings yet
- Pediatric Malignant Bone TumoursDocument28 pagesPediatric Malignant Bone TumourscorneliusNo ratings yet
- Background Case DescriptionDocument1 pageBackground Case DescriptionArli SuryaNo ratings yet
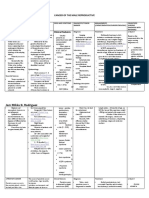
- Understanding Cancer of the Male Reproductive SystemDocument12 pagesUnderstanding Cancer of the Male Reproductive SystemDinarkram Rabreca EculNo ratings yet
- Nonvestibular Schwannoma Tumors in The CPA GgodDocument12 pagesNonvestibular Schwannoma Tumors in The CPA GgodnabilaNo ratings yet
- Spinal Tumor StrongDocument45 pagesSpinal Tumor StrongbettyNo ratings yet
- Spinal Cord TumoursDocument15 pagesSpinal Cord TumoursSakshi NegiNo ratings yet
- Veterinary Oncology, A Short TextbookDocument6 pagesVeterinary Oncology, A Short TextbookMacarena Beatriz Piña ValenciaNo ratings yet
- Intramedullary Osteosarcoma - Pathology - OrthobulletsDocument6 pagesIntramedullary Osteosarcoma - Pathology - OrthobulletsEmiel AwadNo ratings yet
- Peadiatric Brain Tumour: Wong Ann Cheng MD (Ukm) MRCPCH (Uk)Document48 pagesPeadiatric Brain Tumour: Wong Ann Cheng MD (Ukm) MRCPCH (Uk)An Zheng100% (4)
- Bone and Joint TumoursDocument49 pagesBone and Joint TumoursMahmoud Abu Al Amrain100% (1)
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- 2a2. Malignant Bone Tumours - Olatunji O.KDocument37 pages2a2. Malignant Bone Tumours - Olatunji O.KOsifo EmmanuelNo ratings yet
- Soft tissue sarcoma overviewDocument123 pagesSoft tissue sarcoma overviewOana BarbuNo ratings yet
- 6.musculoskeletal TumorsDocument110 pages6.musculoskeletal Tumorslina jamalNo ratings yet
- Lung Tumour Types and CausesDocument7 pagesLung Tumour Types and CausesNestley TiongsonNo ratings yet
- Nose Sinus CA Slides 040519Document40 pagesNose Sinus CA Slides 040519AchmadPrihadiantoNo ratings yet
- Clinical Practice 4: RadiotherapyDocument46 pagesClinical Practice 4: RadiotherapyallordNo ratings yet
- Skin Cancer: No Conflicts of Interest To DiscloseDocument44 pagesSkin Cancer: No Conflicts of Interest To DiscloseKristopher OwensNo ratings yet
- Musculoskeletal ChartsDocument27 pagesMusculoskeletal Chartssurviving nursing school100% (3)
- Musculoskeletal Cancer Surgery - Malawer PDFDocument592 pagesMusculoskeletal Cancer Surgery - Malawer PDFanggita100% (1)
- Bone and Soft Tissue Sarcoma SugarbakerDocument34 pagesBone and Soft Tissue Sarcoma Sugarbakerchindy sulistyNo ratings yet
- Klasifikasi Tumor Otak Menurut WHO 2007 dan 2016Document30 pagesKlasifikasi Tumor Otak Menurut WHO 2007 dan 2016novy rosalia chandraNo ratings yet
- Cellular AberrationDocument83 pagesCellular AberrationA. Lizette PabloNo ratings yet
- Necrotizing EnterocolitisDocument6 pagesNecrotizing EnterocolitisCharlie65129No ratings yet
- ExamsDocument39 pagesExamsCharlie65129No ratings yet
- Management of The Third Stage of Labor: de FinitionDocument6 pagesManagement of The Third Stage of Labor: de FinitionCharlie65129No ratings yet
- Introduction and Basic Principles: Shad DeeringDocument3 pagesIntroduction and Basic Principles: Shad DeeringCharlie65129No ratings yet
- 1617428425599992Document13 pages1617428425599992Charlie65129No ratings yet
- Ultrasound reveals gallstones in asymptomatic womanDocument8 pagesUltrasound reveals gallstones in asymptomatic womanCharlie65129No ratings yet
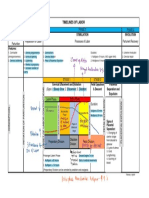
- Timelines of Labor: Phase 1 Phase 2 Phase 4 Prelude To Parturition Preparation For Labor Parturient Recovery Phase 3Document1 pageTimelines of Labor: Phase 1 Phase 2 Phase 4 Prelude To Parturition Preparation For Labor Parturient Recovery Phase 3Charlie65129No ratings yet
- Gallstone Panc TXDocument2 pagesGallstone Panc TXCharlie65129No ratings yet
- Ballard ScoreDocument1 pageBallard ScoreFikriyah FuadiyahNo ratings yet
- Nitrogen Is The Most Common Element in EarthDocument2 pagesNitrogen Is The Most Common Element in EarthCharlie65129No ratings yet
- Catechism of Saint Pope Piux X, The - St. Pius XDocument115 pagesCatechism of Saint Pope Piux X, The - St. Pius XPedro Henrique Gouvêa CoelhoNo ratings yet
- Aagl Practice Guidelines For The Diagnosis and Management of Submucous LeiomyomasDocument20 pagesAagl Practice Guidelines For The Diagnosis and Management of Submucous LeiomyomasCharlie65129No ratings yet
- CPG On Dengue in Children 2017Document108 pagesCPG On Dengue in Children 2017Hannah LeiNo ratings yet
- PGI PHYSIOLOGY EXAM PREPDocument1 pagePGI PHYSIOLOGY EXAM PREPCharlie65129No ratings yet
- WebsitesDocument3 pagesWebsitesCharlie65129No ratings yet
- Puerperium (Trans)Document7 pagesPuerperium (Trans)Charlie65129No ratings yet
- Example Paragraph With CitationsDocument1 pageExample Paragraph With CitationsCharlie65129No ratings yet
- Questions of PancreatitisDocument1 pageQuestions of PancreatitisCharlie65129No ratings yet
- Example Paragraph With CitationsDocument1 pageExample Paragraph With CitationsCharlie65129No ratings yet
- 2 Lawrence MutaleDocument55 pages2 Lawrence MutaleKana FajarNo ratings yet
- Nitrogen Is The Most Common Element in EarthDocument2 pagesNitrogen Is The Most Common Element in EarthCharlie65129No ratings yet
- SbarDocument3 pagesSbarCharlie65129No ratings yet
- Gallstone Panc TXDocument2 pagesGallstone Panc TXCharlie65129No ratings yet
- Chapter Summary - PANCREAS Final (Schwartz) PDFDocument19 pagesChapter Summary - PANCREAS Final (Schwartz) PDFMiguel Cuevas DolotNo ratings yet
- Chronic CalcDocument2 pagesChronic CalcCharlie65129No ratings yet
- 1617428425599992Document13 pages1617428425599992Charlie65129No ratings yet
- ABG ATS Approach Pdf-Notes 201901281644Document36 pagesABG ATS Approach Pdf-Notes 201901281644Charlie65129No ratings yet
- STROKE 3.1 Use of Pharmacologic AgentsDocument1 pageSTROKE 3.1 Use of Pharmacologic AgentsCharlie65129No ratings yet
- Clinical Presentation and Treatment of Carcinoma of Unknown Primary (CUPDocument1 pageClinical Presentation and Treatment of Carcinoma of Unknown Primary (CUPCharlie65129No ratings yet
- AWB DHL Malika BEri PDFDocument3 pagesAWB DHL Malika BEri PDFShipping JenggalaNo ratings yet
- Leyte Department of Education Personal Development DocumentDocument2 pagesLeyte Department of Education Personal Development DocumentMaricar Cesista NicartNo ratings yet
- Paul's View of Justification and Last JudgmentDocument13 pagesPaul's View of Justification and Last JudgmentMik3reyesNo ratings yet
- Principles and Stategies in Teaching MathDocument35 pagesPrinciples and Stategies in Teaching MathGeraldine RamosNo ratings yet
- 15.900 Competitve Strategy MITDocument7 pages15.900 Competitve Strategy MITBrijNo ratings yet
- 4Ps of LifebuoyDocument5 pages4Ps of LifebuoyApurva Saini100% (1)
- Purposive Communication - WK 3Document7 pagesPurposive Communication - WK 3Alexandre QuintoNo ratings yet
- Multiple Bond in CovalentDocument24 pagesMultiple Bond in CovalentAshly GonNo ratings yet
- Science Lesson PlanDocument12 pagesScience Lesson Plananon-695529100% (21)
- Faith and Fascination of A or Ammonite FossilsDocument3 pagesFaith and Fascination of A or Ammonite FossilsRavi UpadhyaNo ratings yet
- Sorting Lesson PlanDocument4 pagesSorting Lesson PlanStasha DuttNo ratings yet
- Political Science Paper Analyzes Society and Polity in IndiaDocument231 pagesPolitical Science Paper Analyzes Society and Polity in IndiaAhmed0% (1)
- Controllogix Enhanced Redundancy System: User ManualDocument254 pagesControllogix Enhanced Redundancy System: User ManualCristian RomeroNo ratings yet
- BadjaoDocument3 pagesBadjaochristianpauloNo ratings yet
- Understanding Application ReasoningDocument42 pagesUnderstanding Application ReasoningadeNo ratings yet
- Scaffolding Load Bearing CapacityDocument1 pageScaffolding Load Bearing CapacityGanga Daran100% (4)
- Cainta Catholic College: Senior High School DepartmentDocument17 pagesCainta Catholic College: Senior High School DepartmentAllan Santos SalazarNo ratings yet
- Nursing Care PlanDocument12 pagesNursing Care Planzsazsageorge86% (21)
- MCQ OpthalmologyDocument45 pagesMCQ OpthalmologyMuhdZaeed100% (1)
- Scada/Ems/Dms: Electric Utilities Networks & MarketsDocument12 pagesScada/Ems/Dms: Electric Utilities Networks & MarketsdoquocdangNo ratings yet
- 5th Grade 13-14 Math Common Core Standards by QuarterDocument3 pages5th Grade 13-14 Math Common Core Standards by QuartermrkballNo ratings yet
- JO1 Plar GIE and MIEDocument2 pagesJO1 Plar GIE and MIEKaloy PlarNo ratings yet
- SAP & ERP Introduction: Centralized ApplicationsDocument6 pagesSAP & ERP Introduction: Centralized ApplicationsMesumNo ratings yet
- Retained Earnings: Appropriation and Quasi-ReorganizationDocument25 pagesRetained Earnings: Appropriation and Quasi-ReorganizationtruthNo ratings yet
- Costa, António Pedro, Luís Paulo Reis, António Moreira. 2019. (Advances in Intelligent Systems and Computing 861) Computer Supported Qualitative Research - New Trends On Qualitative Research-SpringerDocument330 pagesCosta, António Pedro, Luís Paulo Reis, António Moreira. 2019. (Advances in Intelligent Systems and Computing 861) Computer Supported Qualitative Research - New Trends On Qualitative Research-SpringerClarisse ReinfildNo ratings yet
- Flouris-2010-Prediction of VO2maxDocument4 pagesFlouris-2010-Prediction of VO2maxBumbum AtaunNo ratings yet
- Sundqvist 2011 Review McKayDocument7 pagesSundqvist 2011 Review McKaySuriia SeyfullahNo ratings yet
- Adjectives Interconversion of The Degrees of Comparison (Worksheet 3-) Rewrite Each Sentence Using The Other Two Degrees of ComparisonDocument2 pagesAdjectives Interconversion of The Degrees of Comparison (Worksheet 3-) Rewrite Each Sentence Using The Other Two Degrees of ComparisonJeanNo ratings yet
- IN Contemporary World: Student's NameDocument9 pagesIN Contemporary World: Student's NameJessan Ybañez JoreNo ratings yet
- Darood e LakhiDocument5 pagesDarood e LakhiTariq Mehmood Tariq80% (5)