You might also like
- 1 - Intro OpathDocument5 pages1 - Intro Opathcath.rada17No ratings yet
- Oncologic Nursing PDFDocument4 pagesOncologic Nursing PDFDenesa Joyce BustamanteNo ratings yet
- URO 3 - Neoplasm in The Genitourinary TractDocument8 pagesURO 3 - Neoplasm in The Genitourinary TractHa Jae kyeongNo ratings yet
- NeoplasiaDocument78 pagesNeoplasiageetikaNo ratings yet
- CancerDocument18 pagesCanceralexngNo ratings yet
- Y1.6 Neoplasia - Malignant Tumors 2022 PDFDocument41 pagesY1.6 Neoplasia - Malignant Tumors 2022 PDFlina hossamNo ratings yet
- Histopathology of Oral Epithelial TumorsDocument44 pagesHistopathology of Oral Epithelial TumorsRanjit DanielNo ratings yet
- Dermatology SummariesDocument7 pagesDermatology SummariesShiv KolheNo ratings yet
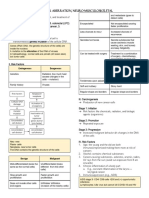
- NCM 106 Cellular-AberrationDocument6 pagesNCM 106 Cellular-AberrationJoanne TolopiaNo ratings yet
- Notes DermaDocument17 pagesNotes DermaCiullaeNo ratings yet
- 02.22.1 Neoplasia I Final PDFDocument79 pages02.22.1 Neoplasia I Final PDFSameeha AbbasNo ratings yet
- Red Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenDocument3 pagesRed Vascular: Polygonal Cells Growing in Nests or Cords Lamellae of Dense CollagenMaryam FadahNo ratings yet
- 5 4b Childhood Malignancy Part 2 DR Melanie Victoria G DarDocument7 pages5 4b Childhood Malignancy Part 2 DR Melanie Victoria G DarSamatha SamathaNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Neoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalDocument4 pagesNeoplasms of Lung, Pleura, and Mediastinum Classification Disease Etiology Epidemiology Pathology ClinicalMrSomnambululNo ratings yet
- Malignant Skin LesionsDocument26 pagesMalignant Skin LesionsdinahzrNo ratings yet
- (Basic Surg A) Oncology-Dr. Acuna (Sleepy Crammers)Document3 pages(Basic Surg A) Oncology-Dr. Acuna (Sleepy Crammers)Mildred DagaleaNo ratings yet
- Tumors of The Orbit by Dr. Jonathan Del Prado 082708Document3 pagesTumors of The Orbit by Dr. Jonathan Del Prado 082708CitrusNo ratings yet
- Rangkuman TumorDocument31 pagesRangkuman TumorraishapiNo ratings yet
- General Stages and TX of Malignant Cells? Naming TumorsDocument11 pagesGeneral Stages and TX of Malignant Cells? Naming TumorsRyan TurnerNo ratings yet
- Surgical Pathology - Major and Minor Salivary GlandsDocument2 pagesSurgical Pathology - Major and Minor Salivary GlandsIsabel CastilloNo ratings yet
- Dermatology - Skin NeoplasmsDocument12 pagesDermatology - Skin NeoplasmsIsabel CastilloNo ratings yet
- TUMOR MATA FX TranslateDocument34 pagesTUMOR MATA FX TranslateAisyahNo ratings yet
- 72 - Skin CancerDocument1 page72 - Skin CancerRica Alyssa PepitoNo ratings yet
- Skin PathologyDocument1 pageSkin PathologySean KeenanNo ratings yet
- C13. Vaginal, Vulvar & CervicalDocument4 pagesC13. Vaginal, Vulvar & Cervicalhari dharshanNo ratings yet
- Malignant Epithelial Slides-1Document5 pagesMalignant Epithelial Slides-1Cenonina Paola TapiaNo ratings yet
- Bladder tumor pathology guideDocument11 pagesBladder tumor pathology guidePankaj DubeyNo ratings yet
- Lecture 3 Ovarian PathologiesDocument5 pagesLecture 3 Ovarian Pathologiesslmsmn101No ratings yet
- General Pathology Midterm ReviewDocument19 pagesGeneral Pathology Midterm ReviewKryss Renato Engel BartolomeNo ratings yet
- Pathology Of: NeoplasiaDocument23 pagesPathology Of: NeoplasiaBryan de GuzmanNo ratings yet
- Neoplasm LectureDocument23 pagesNeoplasm LectureRianNo ratings yet
- Cutaneous Melanoma and Nonmelanoma Skin CancersDocument31 pagesCutaneous Melanoma and Nonmelanoma Skin CancersNice YouNo ratings yet
- Lung Tumour Types and CausesDocument7 pagesLung Tumour Types and CausesNestley TiongsonNo ratings yet
- BENIGN & MALIGNANT LESIONS OF THE SKIN by AlbraaDocument7 pagesBENIGN & MALIGNANT LESIONS OF THE SKIN by AlbraaZoi PapadatouNo ratings yet
- Malignant Tumor: 1. Basal Cell CarcinomaDocument3 pagesMalignant Tumor: 1. Basal Cell CarcinomaERIKA MARIZ DELOS SANTOSNo ratings yet
- Surgery Subspecialty - Skin CancerDocument2 pagesSurgery Subspecialty - Skin CancerJonathan AiresNo ratings yet
- 5 NeoplasiaDocument55 pages5 Neoplasiaadinda kerenNo ratings yet
- Path Adrenal TumorDocument4 pagesPath Adrenal TumorRama HijaziNo ratings yet
- Benign Disease of Vulva and Vagina - FavDocument2 pagesBenign Disease of Vulva and Vagina - FavjeccomNo ratings yet
- Skin CancerDocument7 pagesSkin Cancerعبدالعزيز احمد علي عتشNo ratings yet
- Cellular AberrationDocument6 pagesCellular AberrationNeslie Lagare SamonteNo ratings yet
- Neoplasia and Carcinogenesis ReviewDocument10 pagesNeoplasia and Carcinogenesis Reviewhippypsyduck mdNo ratings yet
- 6 NeoplasiaDocument76 pages6 NeoplasiaMahnoor AyeshaNo ratings yet
- Sarcomas: Bone Sarcoma Soft Tissue SarcomasDocument3 pagesSarcomas: Bone Sarcoma Soft Tissue SarcomasCharlie65129No ratings yet
- Djohan2010bening&malignan TumorDocument13 pagesDjohan2010bening&malignan TumorkikiNo ratings yet
- Screenshot 2023-03-01 at 3.14.03 PMDocument17 pagesScreenshot 2023-03-01 at 3.14.03 PMmohameeedar1No ratings yet
- (GYNE) Ovarian Neoplasms-Dr. Delos Reyes (MRA)Document9 pages(GYNE) Ovarian Neoplasms-Dr. Delos Reyes (MRA)adrian kristopher dela cruzNo ratings yet
- SurgeryDocument35 pagesSurgery2fxs64h4crNo ratings yet
- NeoplasiaDocument31 pagesNeoplasiaAnin PrakashNo ratings yet
- Sinonasal/Nasopharyngeal Tumors: BenignDocument9 pagesSinonasal/Nasopharyngeal Tumors: BenignIsa EnacheNo ratings yet
- Neoplasm Lecture NotesDocument6 pagesNeoplasm Lecture Notesmiguel gaquitNo ratings yet
- Notes: Non-Urothelial Bladder CancersDocument5 pagesNotes: Non-Urothelial Bladder CancersTrivedi NisargNo ratings yet
- ONCOLOGYDocument26 pagesONCOLOGYShawn TejanoNo ratings yet
- Tumor of The EyeDocument40 pagesTumor of The EyeGustiAngriAngalanNo ratings yet
- Eca - Cellular Aberration-Neuro-MusculoskeletalDocument29 pagesEca - Cellular Aberration-Neuro-MusculoskeletalFrancis Alfred EscaranNo ratings yet
- Topic List - Tumor Kulit: Pembimbing: Dr. Asep Tajul Mutaqin, Sp. BDocument50 pagesTopic List - Tumor Kulit: Pembimbing: Dr. Asep Tajul Mutaqin, Sp. BMarcia CiaNo ratings yet
- Lecture, 9Document38 pagesLecture, 9محمد ربيعيNo ratings yet
- Dermatology Notes for Medical StudentsFrom EverandDermatology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (5)
- Horne 2018Document11 pagesHorne 2018Martga Bella RahimiNo ratings yet
- What is Cancer? Understanding the DiseaseDocument5 pagesWhat is Cancer? Understanding the DiseaseElijah Loh Keng SoonNo ratings yet
- Announcement SGU 2021Document10 pagesAnnouncement SGU 2021ceciliaNo ratings yet
- A221505 "RT CHARM Trial": Dana Koller, CMD, RT (T)Document20 pagesA221505 "RT CHARM Trial": Dana Koller, CMD, RT (T)api-456373408No ratings yet
- The Burying Grandma Example College EssayDocument4 pagesThe Burying Grandma Example College EssayArfa IrfanNo ratings yet
- Inquiries, Investigation, and Immersion: Quarter 2 Module 2 - Lesson 4Document14 pagesInquiries, Investigation, and Immersion: Quarter 2 Module 2 - Lesson 4fio jennNo ratings yet
- Mixed Müllerian Tumor of UterusDocument3 pagesMixed Müllerian Tumor of UterusInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Oncology McqsDocument115 pagesOncology McqsSyed NoorNo ratings yet
- Psycho-Oncology - 2018 - Die Trill - Jimmie Holland The Founder Developer and The Soul of The InternationalDocument3 pagesPsycho-Oncology - 2018 - Die Trill - Jimmie Holland The Founder Developer and The Soul of The InternationalReginaNo ratings yet
- EURAMOSDocument77 pagesEURAMOSvural kesikNo ratings yet
- Set 2Document6 pagesSet 2atiqah90No ratings yet
- 2017 ESMO Essentials For Clinicians Gynaecological TumoursDocument100 pages2017 ESMO Essentials For Clinicians Gynaecological TumoursMaria RamosNo ratings yet
- Tesis RomanosNanclares21Document348 pagesTesis RomanosNanclares21Evelyn MedelNo ratings yet
- WJCC 3 231Document15 pagesWJCC 3 231byk5s82mwnNo ratings yet
- The Memorial SymptomDocument10 pagesThe Memorial SymptomChristine SiburianNo ratings yet
- Cervical Cancer Screening and Occurrence TrendsDocument109 pagesCervical Cancer Screening and Occurrence TrendsVincent eneNo ratings yet
- NCLEX CancerDocument70 pagesNCLEX Cancermanhua fanaticNo ratings yet
- Anticancer Claims of Health Supplement QuestionedDocument6 pagesAnticancer Claims of Health Supplement QuestionedNnNo ratings yet
- Farmakoterapi Infeksi, Kanker, Dan Gangguan Nutrisi Self-Assessment Question AnticancerDocument7 pagesFarmakoterapi Infeksi, Kanker, Dan Gangguan Nutrisi Self-Assessment Question AnticancerRAPER HMF 2019No ratings yet
- Gu MDT 1Document14 pagesGu MDT 1Emy FrancisNo ratings yet
- Short Report: G. Catimel, F. Chauvin, J. P. Guastalla, P. Rebattu, P. B I R o N M. ClavelDocument3 pagesShort Report: G. Catimel, F. Chauvin, J. P. Guastalla, P. Rebattu, P. B I R o N M. ClavelApril NNo ratings yet
- Kura PatentDocument65 pagesKura PatentCharles GrossNo ratings yet
- Veterinary: Endoscopic Accessories Solu OnDocument2 pagesVeterinary: Endoscopic Accessories Solu OnXD MNo ratings yet
- Assessment of Sun-Related Behaviour, Knowledge and Attitudes Among Nursing StudentsDocument9 pagesAssessment of Sun-Related Behaviour, Knowledge and Attitudes Among Nursing StudentsAdrian Alexis Romero GuillenNo ratings yet
- Extravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsDocument12 pagesExtravasation Neutral (Non-Irritant) Irritant Irritant With Vesicant Properties VesicantsmarcNo ratings yet
- Cancer Chemotherapy - A Critical Analysis of Its 60 Years of HistoryDocument19 pagesCancer Chemotherapy - A Critical Analysis of Its 60 Years of HistoryCarlaValongoNo ratings yet
- BRAF Gene Mutation TestsDocument5 pagesBRAF Gene Mutation TestsCota AncutaNo ratings yet
- Global Citizen EssayDocument1 pageGlobal Citizen Essayapi-544791862No ratings yet
- Mammography: Quality Control ManualDocument360 pagesMammography: Quality Control ManualSara Bustillos BuenañoNo ratings yet
- Colorectal Cancer Liver MetastasisDocument18 pagesColorectal Cancer Liver Metastasisjmiller623No ratings yet