You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The LOLCat Bible - The Book of Genesis (Rev2)Document39 pagesThe LOLCat Bible - The Book of Genesis (Rev2)Reese Johnson100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- GTC Export Matrix Q1 011617 - Final LockedDocument11 pagesGTC Export Matrix Q1 011617 - Final LockednboninaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Systems Thinking BookDocument42 pagesSystems Thinking BookArturo Andres100% (4)
- Soal Inggris-1Document8 pagesSoal Inggris-1Rigel n drum0% (1)
- 8.TotalLube911 MSDSDocument2 pages8.TotalLube911 MSDSGuillermo DamianNo ratings yet
- Section Iv - TS2 Aa0851403Document79 pagesSection Iv - TS2 Aa0851403REYNOLD VALVESNo ratings yet
- Manual XORO en HRS8664 HRS8660 HRS8659 HRS8658 HRS8566v2 HRS8556v2 HRS2610Document40 pagesManual XORO en HRS8664 HRS8660 HRS8659 HRS8658 HRS8566v2 HRS8556v2 HRS2610Aaa AaNo ratings yet
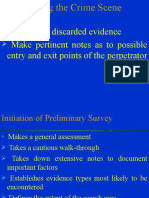
- Crime Scene Search BDocument41 pagesCrime Scene Search BJoshua ReyesNo ratings yet
- Formato de Pedido PDFDocument10 pagesFormato de Pedido PDFELIAZAR TORREZNo ratings yet
- Global Health Estimates 2019 Summary Tables: Deaths by Cause, Age and Sex, by World Bank Income Group, 2000-2019Document42 pagesGlobal Health Estimates 2019 Summary Tables: Deaths by Cause, Age and Sex, by World Bank Income Group, 2000-2019DanielaNo ratings yet
- Traing ReportDocument38 pagesTraing ReportBhanwar BamniaNo ratings yet
- Umberto Eco, Anthony Oldcorn - From The Tree To The Labyrinth - Historical Studies On The Sign and Interpretation - Harvard University Press (2014)Document640 pagesUmberto Eco, Anthony Oldcorn - From The Tree To The Labyrinth - Historical Studies On The Sign and Interpretation - Harvard University Press (2014)JughrtaActifAbuNawwas100% (1)
- MX25U6473FDocument90 pagesMX25U6473FSusan KusumhiyaNo ratings yet
- CBM2092 DatasheetDocument18 pagesCBM2092 DatasheetGauravNo ratings yet
- Platelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Document6 pagesPlatelet Von Willebrand Factor in Hermansky-Pudlak Syndrome (American Journal of Hematology, Vol. 59, Issue 2) (1998)Ahmed MagzoubNo ratings yet
- Rolls Royce / Bentley Service Handbook 1955Document1,283 pagesRolls Royce / Bentley Service Handbook 1955head_masterNo ratings yet
- FRMP11S SPB203Document13 pagesFRMP11S SPB203jyapias_1No ratings yet
- Datasheet - KTQM77 - mITXDocument2 pagesDatasheet - KTQM77 - mITXalexandru_mg3No ratings yet
- Houses & SignsDocument8 pagesHouses & SignsShivarubhanNo ratings yet
- Truss 6 V - Plate Connection DesignDocument9 pagesTruss 6 V - Plate Connection DesignSiddharth Tiwari100% (1)
- Auto Selection of Any Available Phase, in 3 Phase Supply System-Ijaerdv05i10703Document9 pagesAuto Selection of Any Available Phase, in 3 Phase Supply System-Ijaerdv05i10703Bøññïe Ådë Cöloñêl100% (1)
- 11th STD - Class-4 (ZMP Sir) - Chemical Coordination and Integration - NotesDocument16 pages11th STD - Class-4 (ZMP Sir) - Chemical Coordination and Integration - Notesdisha shuklaNo ratings yet
- Experimental and Analytical Investigation of Service-Load Stresses in Cellular Beams - AspDocument2 pagesExperimental and Analytical Investigation of Service-Load Stresses in Cellular Beams - Aspchristos032No ratings yet
- Feasibility Study of Hexane ProductionDocument3 pagesFeasibility Study of Hexane ProductionIntratec SolutionsNo ratings yet
- Test 1 StatsDocument7 pagesTest 1 StatsLANo ratings yet
- Paper 1 - Set B 15 National Certification Examination FOR Energy Managers & Energy Auditors - August, 2014Document19 pagesPaper 1 - Set B 15 National Certification Examination FOR Energy Managers & Energy Auditors - August, 2014Soumya RanjanNo ratings yet
- Hand-Powered Ultralow-Cost Paper CentrifugeDocument22 pagesHand-Powered Ultralow-Cost Paper CentrifugeSanyogita RaniNo ratings yet
- Take Home Assignment of MEOW: PHY F111Document1 pageTake Home Assignment of MEOW: PHY F111renu chawlaNo ratings yet
- Low Voltage Duct Banks: Key PlanDocument1 pageLow Voltage Duct Banks: Key PlanFathy RamadanNo ratings yet
- Sylvania 1986 Large Lamp Ordering GuideDocument88 pagesSylvania 1986 Large Lamp Ordering GuideAlan Masters100% (2)