You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5811)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- NV10USB Software Implementation GuideDocument26 pagesNV10USB Software Implementation GuideApple Pie100% (1)
- Endoscopic Resection (Endoscopic Mucosal Resection Endoscopic Submucosaldissection) For Superficial Esophageal Squamous Cell Carcinoma Current Status of Various TecDocument7 pagesEndoscopic Resection (Endoscopic Mucosal Resection Endoscopic Submucosaldissection) For Superficial Esophageal Squamous Cell Carcinoma Current Status of Various TecDiego EskinaziNo ratings yet
- 2.1. Anti-CTLA-4 Antibody Therapy Immune Monitoring During Clinical Development of A Novel ImmunotherapyDocument19 pages2.1. Anti-CTLA-4 Antibody Therapy Immune Monitoring During Clinical Development of A Novel ImmunotherapyDiego EskinaziNo ratings yet
- 2.2. Cancer Immunotherapy Co-Stimulatory Agonists and Co-Inhibitory AntagonistsDocument11 pages2.2. Cancer Immunotherapy Co-Stimulatory Agonists and Co-Inhibitory AntagonistsDiego EskinaziNo ratings yet
- GLOBOCAN Argentina 2018Document2 pagesGLOBOCAN Argentina 2018Diego EskinaziNo ratings yet
- 1.4. RB Mitotic Implications of A Tumor Suppressor - Nat Rev CancerDocument15 pages1.4. RB Mitotic Implications of A Tumor Suppressor - Nat Rev CancerDiego EskinaziNo ratings yet
- Surgical Oncology in Europe - 2004Document5 pagesSurgical Oncology in Europe - 2004Diego EskinaziNo ratings yet
- Van Der Speeten Et Al. - Current Practice in Delivering HIPEC, EPIC and NIPSDocument10 pagesVan Der Speeten Et Al. - Current Practice in Delivering HIPEC, EPIC and NIPSDiego EskinaziNo ratings yet
- 7 of The Most Important Metrics For Measuring or EfficiencyDocument4 pages7 of The Most Important Metrics For Measuring or EfficiencyDiego EskinaziNo ratings yet
- Basic Principles in Surgical Oncology - Cady1997 Arch Surg PDFDocument9 pagesBasic Principles in Surgical Oncology - Cady1997 Arch Surg PDFDiego EskinaziNo ratings yet
- CRS and HIPEC in Patients With PC - Yang Et Al. Jgo-2019 PDFDocument15 pagesCRS and HIPEC in Patients With PC - Yang Et Al. Jgo-2019 PDFDiego EskinaziNo ratings yet
- Project Shear Wall 1Document13 pagesProject Shear Wall 1nkjm rtdtNo ratings yet
- ImmediacyDocument2 pagesImmediacyPantatNyanehBurikNo ratings yet
- 22 - II - Tennet - Werkplan EngDocument165 pages22 - II - Tennet - Werkplan EngJuan Pablo Wilches ArboledaNo ratings yet
- CS8251-Programming in CDocument14 pagesCS8251-Programming in COmprakash DNo ratings yet
- Science 8 LP 2Document6 pagesScience 8 LP 2Judilyn Llamas LabendiaNo ratings yet
- Charmander Amigurumi Free Patter1Document9 pagesCharmander Amigurumi Free Patter1fhdfccbNo ratings yet
- An Introduction To The Mckenzie Method: Treating Your Own BackDocument24 pagesAn Introduction To The Mckenzie Method: Treating Your Own BackR HariNo ratings yet
- PhySci - Q2 - M4 - Properties of Light and Wave Like - Properties of Electron - v5Document19 pagesPhySci - Q2 - M4 - Properties of Light and Wave Like - Properties of Electron - v5genie lagunayNo ratings yet
- Rule of Law and Indian PolityDocument6 pagesRule of Law and Indian PolityJalaj AgarwalNo ratings yet
- Case Study)Document2 pagesCase Study)Chin FiguraNo ratings yet
- CSS Bridge Group - Guidance Document - Parts A, B1, B2, B3 and CDocument152 pagesCSS Bridge Group - Guidance Document - Parts A, B1, B2, B3 and CAlejandro MateoNo ratings yet
- Senior High School Module (Week 5 - Media)Document7 pagesSenior High School Module (Week 5 - Media)Maestro Lazaro100% (2)
- Astm c1461Document4 pagesAstm c1461Júlio RosaNo ratings yet
- Mobile Gaming: Its Influence To A Senior High School Academic Performance in Online LearningDocument18 pagesMobile Gaming: Its Influence To A Senior High School Academic Performance in Online LearningReenieNo ratings yet
- Artículo - BCG - The Most Innovative Companies PDFDocument20 pagesArtículo - BCG - The Most Innovative Companies PDFcasoreyNo ratings yet
- Examguide3 202210041702Document43 pagesExamguide3 20221004170299710114003aNo ratings yet
- MPDFDocument10 pagesMPDFRio BahouxNo ratings yet
- Developmental PsychologyDocument15 pagesDevelopmental PsychologyJSeashark0% (1)
- Probability 1Document64 pagesProbability 1Deepak Kumar Arora100% (3)
- Traditional Mediterranean Architecture: Riwaq HouseDocument5 pagesTraditional Mediterranean Architecture: Riwaq HousefofiNo ratings yet
- Φ45 AC Tubular MotorDocument4 pagesΦ45 AC Tubular MotorwistarmotorNo ratings yet
- GK Build Instructions v4-2 PDFDocument11 pagesGK Build Instructions v4-2 PDFMoogNo ratings yet
- Harmonographs. II. Circular DesignDocument10 pagesHarmonographs. II. Circular DesignAditama MKNo ratings yet
- KadizadeliDocument350 pagesKadizadeliJormandoAndradeNo ratings yet
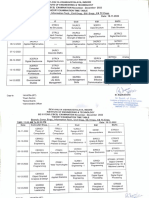
- Exam Time Table Nov 19, 2022Document6 pagesExam Time Table Nov 19, 2022Motive to MotivateNo ratings yet
- CounselLink - Law Department Budgeting and ForecastingDocument12 pagesCounselLink - Law Department Budgeting and ForecastingBuddhika PereraNo ratings yet
- How To Keep & Motivate Your Qa Team - Without Increasing Your Budget - Marina Gil Santa MariaDocument8 pagesHow To Keep & Motivate Your Qa Team - Without Increasing Your Budget - Marina Gil Santa Mariavaraprasad119No ratings yet
- Hardware Assignment 1Document3 pagesHardware Assignment 1Timvane Tim C Chabaluka0% (1)