You might also like
- Hospital Policy ManualDocument26 pagesHospital Policy ManualBasant GuptaNo ratings yet
- MIS in HospitalDocument64 pagesMIS in Hospitalabinthevarmadom87% (15)
- Safe Hospitals AssessmentDocument74 pagesSafe Hospitals AssessmentJB Myrrh Sta Romana100% (1)
- QA For Radiology DepartmentDocument3 pagesQA For Radiology DepartmentRaviraj Pishe100% (1)
- Revised EMS Run SheetDocument2 pagesRevised EMS Run Sheetanon-939227100% (2)
- Improving Healthcare Through Advocacy: A Guide for the Health and Helping ProfessionsFrom EverandImproving Healthcare Through Advocacy: A Guide for the Health and Helping ProfessionsNo ratings yet
- Hca 468 PaperDocument9 pagesHca 468 Paperapi-487927401No ratings yet
- PRC-BoN Core Competency Standards - Nle Test Framework.06.07.sDocument43 pagesPRC-BoN Core Competency Standards - Nle Test Framework.06.07.sjosephine100% (7)
- SNLE Applicant Guide 2020Document14 pagesSNLE Applicant Guide 2020Tati MaryatiNo ratings yet
- Standard Operating Procedures For Pharmaceutical Care Delivery in Health FacilitiesDocument7 pagesStandard Operating Procedures For Pharmaceutical Care Delivery in Health FacilitiesNhu0% (1)
- Nur 460 Capstone Final PaperDocument15 pagesNur 460 Capstone Final Paperapi-429837528No ratings yet
- Customized NQAS Checklist For Non Beded PHC of OdishaDocument40 pagesCustomized NQAS Checklist For Non Beded PHC of Odishaqa100% (1)
- Hospital Emergency Response Checklist EngDocument26 pagesHospital Emergency Response Checklist EngRaniNo ratings yet
- Medical Equipment Management ProgramDocument3 pagesMedical Equipment Management Programyekta8No ratings yet
- Clinical Services Plan TTM SamoaDocument69 pagesClinical Services Plan TTM SamoajohnkornieNo ratings yet
- National Quality Assurance Standards 2020Document76 pagesNational Quality Assurance Standards 2020Jenifer Monica100% (1)
- Hospital Safety PromotionDocument46 pagesHospital Safety PromotionRhodora BenipayoNo ratings yet
- Sound Hospital MGTDocument5 pagesSound Hospital MGThii_bhartiNo ratings yet
- FMEA10 Sample PagesDocument24 pagesFMEA10 Sample Pageswy1suwirjaNo ratings yet
- Structure Indicators of The HospitalDocument4 pagesStructure Indicators of The HospitalJery JsNo ratings yet
- Guidelines On Medical Equipment Management in NigeriaDocument8 pagesGuidelines On Medical Equipment Management in NigeriaBALANo ratings yet
- JCI QUESTIONNAIRE-PCI Dept.Document6 pagesJCI QUESTIONNAIRE-PCI Dept.Rabiya Sajjad100% (2)
- Disaster Preparedness Checklist For HospitalsDocument3 pagesDisaster Preparedness Checklist For HospitalsDnyanesh AitalwadNo ratings yet
- MSQH 5th Edition Draft Standard 5 - Prevention and Control of InfectionDocument22 pagesMSQH 5th Edition Draft Standard 5 - Prevention and Control of InfectionEsmar A. Hamid Kenoh0% (1)
- Medical Equipment Management PolicyDocument13 pagesMedical Equipment Management Policysdroyafmc100% (1)
- The Italian Healthcare SystemDocument5 pagesThe Italian Healthcare SystemAnnamaria FrezzaNo ratings yet
- Inter Hospital Transfer SopDocument2 pagesInter Hospital Transfer SopNATARAJAN RAJENDRANNo ratings yet
- Quality Manager Job Description - 09-13Document3 pagesQuality Manager Job Description - 09-13DrSaswat LincolnNo ratings yet
- Case Study - Lilavati: HospitalDocument39 pagesCase Study - Lilavati: HospitalCharanjeet Singh AroraNo ratings yet
- Medical Staff BylawsDocument39 pagesMedical Staff BylawsMaria Francesca MapaNo ratings yet
- MRD ProjectDocument23 pagesMRD Projectsamgill66916No ratings yet
- Diagnostic X-Ray Imaging Quality AssuranceDocument23 pagesDiagnostic X-Ray Imaging Quality AssurancePrabhsharn singhNo ratings yet
- Of Office of The Secretary: Republic PhilippinesDocument112 pagesOf Office of The Secretary: Republic PhilippinesAlex SanchezNo ratings yet
- A P Policy & Procedure: Ntibiotic OlicyDocument24 pagesA P Policy & Procedure: Ntibiotic Olicyvijay kumarNo ratings yet
- STANDARD OPERATING PROCEDURES For Establishing and Running Key Populations Clinics in KenyaDocument40 pagesSTANDARD OPERATING PROCEDURES For Establishing and Running Key Populations Clinics in KenyaElvisNo ratings yet
- Radiology ServicesDocument5 pagesRadiology Servicesshah007zaadNo ratings yet
- Patient Friendly Standards For AHPIDocument26 pagesPatient Friendly Standards For AHPIdrruchiNo ratings yet
- Hospital Disaster Preparedness Self-Assessment ToolDocument47 pagesHospital Disaster Preparedness Self-Assessment ToolJayvee GuerreroNo ratings yet
- Conference Program: 4th Asia Pacific Regional Conference On Health Impact Assessment (HIA), Seoul, South Korea, 9-11 October 2012Document56 pagesConference Program: 4th Asia Pacific Regional Conference On Health Impact Assessment (HIA), Seoul, South Korea, 9-11 October 2012ADB Health Sector GroupNo ratings yet
- Improve Care.: Empower ChangeDocument13 pagesImprove Care.: Empower Changekukun67% (3)
- HospitalDocument4 pagesHospitalLyka Mendoza MojaresNo ratings yet
- KPI Discussion Paper 3Document22 pagesKPI Discussion Paper 3Manager HR Hijaz Hospital100% (1)
- New Classification of General Hospitals in The Philippines Based On Functional CapacityDocument5 pagesNew Classification of General Hospitals in The Philippines Based On Functional CapacityVer Bautista100% (1)
- Clinical Establishment Act Standards For Hospital (LEVEL 3)Document36 pagesClinical Establishment Act Standards For Hospital (LEVEL 3)bksubrat100% (3)
- Lesson 5 - Electronic Health Record and Clinical Informatics - PPT StudentDocument42 pagesLesson 5 - Electronic Health Record and Clinical Informatics - PPT Studentbeer_ettaaNo ratings yet
- HmisDocument14 pagesHmis166873100% (1)
- A Research On Design of Heating, Ventilation and Air Conditioning of Hygienic Spaces in Hosp PDFDocument145 pagesA Research On Design of Heating, Ventilation and Air Conditioning of Hygienic Spaces in Hosp PDFMAGDY KAMELNo ratings yet
- Activities Patient SafetyDocument13 pagesActivities Patient SafetyummuawisyNo ratings yet
- Saudi TelemedicineDocument80 pagesSaudi TelemedicineVenkata KrishnaNo ratings yet
- Glossary Health TeccnologyDocument4 pagesGlossary Health TeccnologyreneportilloNo ratings yet
- Clinical Procedure Manual-RefDocument80 pagesClinical Procedure Manual-Refrashmi elizabeth easow100% (1)
- Infection Control NHS PolicyDocument12 pagesInfection Control NHS PolicyYahya Salem100% (1)
- Joint Commission International (JCI) Requirements Related To Safe SurgeryDocument16 pagesJoint Commission International (JCI) Requirements Related To Safe Surgeryngurah_wardanaNo ratings yet
- New Assessment Tool For HospitalsDocument60 pagesNew Assessment Tool For HospitalssaguliteNo ratings yet
- Antimicrobial Prescribing PolicyDocument20 pagesAntimicrobial Prescribing PolicycraNo ratings yet
- Challenges For AccreditationDocument22 pagesChallenges For AccreditationMohammad Muntaz AliNo ratings yet
- IPSG PresentationDocument38 pagesIPSG Presentationmuhammed shamaa100% (1)
- Homoeopathy Indicators NABHDocument105 pagesHomoeopathy Indicators NABHMamoni MaityNo ratings yet
- HospitalDocument27 pagesHospitaljyothiNo ratings yet
- Hospital Emergency Operations Plan TemplateDocument53 pagesHospital Emergency Operations Plan TemplateNicholaiCabadduNo ratings yet
- 35.hospital DevelopmentDocument6 pages35.hospital DevelopmentJayson Viscayno LanatNo ratings yet
- Sentinel Events: Vidya PrasadDocument21 pagesSentinel Events: Vidya PrasadTOUSHIFAHEMEDNo ratings yet
- Hospital Wastes Management PlanDocument4 pagesHospital Wastes Management PlanRPh Krishna Chandra Jagrit100% (1)
- Annual Plan: Infection Prevention & Control DepartmentDocument3 pagesAnnual Plan: Infection Prevention & Control DepartmentSherina Edding0% (1)
- MSDS - Health - Final PDFDocument122 pagesMSDS - Health - Final PDFmalikamirshahzad100% (1)
- Patient Safety Organization A Complete Guide - 2020 EditionFrom EverandPatient Safety Organization A Complete Guide - 2020 EditionNo ratings yet
- Bma Consultant Objective ExamplesDocument40 pagesBma Consultant Objective ExamplesKutu MiaNo ratings yet
- Premature Ejaculation Fact SheetDocument2 pagesPremature Ejaculation Fact SheetKutu MiaNo ratings yet
- National Epilepsy Consensus Guideline Society of Neurologists of Bangladesh 1Document130 pagesNational Epilepsy Consensus Guideline Society of Neurologists of Bangladesh 1Kutu MiaNo ratings yet
- National Guideline For Kala-Azar Case Management Bangladesh 2013Document72 pagesNational Guideline For Kala-Azar Case Management Bangladesh 2013Kutu MiaNo ratings yet
- Having A Percutaneous Endoscopic Gastrostomy PEG: Information For PatientsDocument12 pagesHaving A Percutaneous Endoscopic Gastrostomy PEG: Information For PatientsKutu MiaNo ratings yet
- IELTS Speaking Practice Test VideoDocument4 pagesIELTS Speaking Practice Test VideoKutu MiaNo ratings yet
- IELTS Speaking Part 3 TopicsDocument4 pagesIELTS Speaking Part 3 TopicsKutu MiaNo ratings yet
- Fellowship Application Deadlines 2022 2023Document2 pagesFellowship Application Deadlines 2022 2023Kutu MiaNo ratings yet
- Clinical Fellow Funding Income Support GuidelinesDocument1 pageClinical Fellow Funding Income Support GuidelinesKutu MiaNo ratings yet
- Fellowship Program APPLICATION 2020 / 2021: AnesthesiaDocument2 pagesFellowship Program APPLICATION 2020 / 2021: AnesthesiaKutu MiaNo ratings yet
- Ckgs Order Form India VisaDocument2 pagesCkgs Order Form India VisaKutu MiaNo ratings yet
- IELTS Speaking Part 2 Topics QuestionsDocument7 pagesIELTS Speaking Part 2 Topics QuestionsKutu MiaNo ratings yet
- MTI Online Portal - Step by Step GuideDocument3 pagesMTI Online Portal - Step by Step GuideKutu MiaNo ratings yet
- MRCP (UK) RegulationsDocument19 pagesMRCP (UK) RegulationsKutu MiaNo ratings yet
- Part 2 - MRCPUKDocument3 pagesPart 2 - MRCPUKKutu MiaNo ratings yet
- 450 English To EnglishDocument451 pages450 English To EnglishKutu MiaNo ratings yet
- Format - MRCPUKDocument3 pagesFormat - MRCPUKKutu MiaNo ratings yet
- Ataxias Best Practice PDFDocument56 pagesAtaxias Best Practice PDFKutu MiaNo ratings yet
- Hospital Management System For Mayo Clinic: Prepared By: KISHOR KUNALDocument12 pagesHospital Management System For Mayo Clinic: Prepared By: KISHOR KUNALRohit Krishnan MNo ratings yet
- Putri, 2021Document9 pagesPutri, 2021nirmala amirNo ratings yet
- ASHP Hospital Drug Distribution and Control PDFDocument9 pagesASHP Hospital Drug Distribution and Control PDFKita RadisaNo ratings yet
- Promoting Patient Safety: An Ethical Basis For Policy DeliberationDocument20 pagesPromoting Patient Safety: An Ethical Basis For Policy DeliberationThe Hastings CenterNo ratings yet
- Appointment Of: Senior Clinical Fellow in Obstetrics & GynaecologyDocument20 pagesAppointment Of: Senior Clinical Fellow in Obstetrics & GynaecologyOzhenNo ratings yet
- Tele NursingDocument41 pagesTele Nursingcalvin100% (1)
- Clinical Nursing JudgementDocument8 pagesClinical Nursing Judgementapi-546517574No ratings yet
- 53734d Consultant Physician With Interest in Gastroenterology 3 PostsDocument27 pages53734d Consultant Physician With Interest in Gastroenterology 3 PostsShelley CochraneNo ratings yet
- R06031 Adefunke U24Document25 pagesR06031 Adefunke U24Minhaz RahmanNo ratings yet
- Test Bank For Introduction To Health Care Finance and Accounting 1st Edition Carlene Harrison William P HarrisonDocument11 pagesTest Bank For Introduction To Health Care Finance and Accounting 1st Edition Carlene Harrison William P Harrisoncarwynquanh4tuozNo ratings yet
- OBC Mid Term Fall 2020 BBA 2yrs KASBITDocument9 pagesOBC Mid Term Fall 2020 BBA 2yrs KASBITOWAIS AHMED NISAR AHMEDNo ratings yet
- Gloria M. Dela Cruz: Personal DataDocument4 pagesGloria M. Dela Cruz: Personal Datamissglorya100% (1)
- YOTiMES15 PDFDocument380 pagesYOTiMES15 PDFbmc_nehaNo ratings yet
- Remistart Enrollment FormDocument2 pagesRemistart Enrollment FormDerek LemonNo ratings yet
- Afghanistan MRRD Building ManualDocument120 pagesAfghanistan MRRD Building ManualJohn N. Constance100% (1)
- Introduction:-: Ambulatory Healthcare Organizations IntroducedDocument7 pagesIntroduction:-: Ambulatory Healthcare Organizations Introducedanimesh pandaNo ratings yet
- 6.7 NotesDocument9 pages6.7 NoteszufaroaaNo ratings yet
- HospitalDocument24 pagesHospitalrini0026100% (1)
- Adm and DischargeDocument29 pagesAdm and DischargeRekha DehariyaNo ratings yet
- Resume of Yelly2danniDocument1 pageResume of Yelly2danniapi-31704300No ratings yet
- Discharging A ClientDocument6 pagesDischarging A ClientNorman Batalla Juruena, DHCM, PhD, RNNo ratings yet
- Apollo Kavach.: Always On CallDocument16 pagesApollo Kavach.: Always On CallRaghavendra AnanthaNo ratings yet
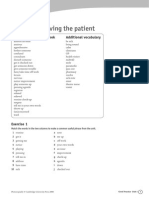
- GoodPractice WL U01ReceivingPatientDocument3 pagesGoodPractice WL U01ReceivingPatientReka Kutasi100% (1)
- Strategies To Promote ConcordanceDocument4 pagesStrategies To Promote ConcordanceDem BertoNo ratings yet