You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Superflex Social Thinking CurriculumDocument25 pagesSuperflex Social Thinking Curriculumcsepulveda10No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Nursing Process Lecture NotesDocument16 pagesNursing Process Lecture NotesReden Ocampo100% (16)
- Baron-Cohen. Undertanding Other Minds PDFDocument517 pagesBaron-Cohen. Undertanding Other Minds PDFJosé Luis Meléndez100% (10)
- Simone de Beauvoir - ScribdDocument3 pagesSimone de Beauvoir - ScribdAshley MalcomNo ratings yet
- The Phenotypic Spectrum of PCDH12 Associated Disor 2022 European Journal ofDocument7 pagesThe Phenotypic Spectrum of PCDH12 Associated Disor 2022 European Journal ofcsepulveda10No ratings yet
- Implementation of Motor Function Measure Score Percent 2022 European JournalDocument6 pagesImplementation of Motor Function Measure Score Percent 2022 European Journalcsepulveda10No ratings yet
- PROMPT Intervention For Children With Severe Speech Motor Delay - A Randomized Control Trial PDFDocument9 pagesPROMPT Intervention For Children With Severe Speech Motor Delay - A Randomized Control Trial PDFcsepulveda10No ratings yet
- The Use of Intrathecal Baclofen For Management of SP 2022 European Journal oDocument5 pagesThe Use of Intrathecal Baclofen For Management of SP 2022 European Journal ocsepulveda10No ratings yet
- Neurophysiological Recordings Improve The Accuracy of 2022 European JournalDocument6 pagesNeurophysiological Recordings Improve The Accuracy of 2022 European Journalcsepulveda10No ratings yet
- Exploring The Connections Between Basal Ganglia and Corte 2022 European JourDocument9 pagesExploring The Connections Between Basal Ganglia and Corte 2022 European Jourcsepulveda10No ratings yet
- Cortical Interactions Underlying The Production of Speech SoundsDocument16 pagesCortical Interactions Underlying The Production of Speech Soundscsepulveda10No ratings yet
- Aba V/S TeacchDocument15 pagesAba V/S Teacchcsepulveda10No ratings yet
- Gates 2017Document58 pagesGates 2017csepulveda10No ratings yet
- ¿Seguridad de La Sucralosa?Document32 pages¿Seguridad de La Sucralosa?csepulveda10No ratings yet
- Fuller 2019Document18 pagesFuller 2019csepulveda10No ratings yet
- El Consumo A Corto Plazo de Sucralosa Con CarbohidratosDocument18 pagesEl Consumo A Corto Plazo de Sucralosa Con Carbohidratoscsepulveda10No ratings yet
- PDFDocument11 pagesPDFahoogma33No ratings yet
- Aba V/S TeacchDocument15 pagesAba V/S Teacchcsepulveda10No ratings yet
- El Consumo A Corto Plazo de Sucralosa Con CarbohidratosDocument18 pagesEl Consumo A Corto Plazo de Sucralosa Con Carbohidratoscsepulveda10No ratings yet
- El Consumo A Corto Plazo de Sucralosa Con CarbohidratosDocument18 pagesEl Consumo A Corto Plazo de Sucralosa Con Carbohidratoscsepulveda10No ratings yet
- Neuropsychological Characteristics of Children With MixedDocument6 pagesNeuropsychological Characteristics of Children With MixedsivitranNo ratings yet
- Epigenetics and Autism PDFDocument10 pagesEpigenetics and Autism PDFcsepulveda10No ratings yet
- 2003 Book IntegratedNeuroscience PDFDocument730 pages2003 Book IntegratedNeuroscience PDFaccrassusNo ratings yet
- Longitudinal Study of Sensory Features in Children With Autism Spectrum DisorderDocument8 pagesLongitudinal Study of Sensory Features in Children With Autism Spectrum DisorderMiguel RomeroNo ratings yet
- Autism Spectrum Disorder Screening Instruments For Very PDFDocument30 pagesAutism Spectrum Disorder Screening Instruments For Very PDFAna Maria Inostroza GarcesNo ratings yet
- Autismo - ¿Un Trastorno Del "Período Crítico"?Document18 pagesAutismo - ¿Un Trastorno Del "Período Crítico"?csepulveda10No ratings yet
- Effect of Epilepsy On Autism Symptoms in Angelman SyndromeDocument8 pagesEffect of Epilepsy On Autism Symptoms in Angelman Syndromecsepulveda10No ratings yet
- Discurso NarrativoDocument12 pagesDiscurso Narrativocsepulveda10No ratings yet
- Autismo - ¿Un Trastorno Del "Período Crítico"?Document18 pagesAutismo - ¿Un Trastorno Del "Período Crítico"?csepulveda10No ratings yet
- Research in Autism Spectrum Disorders: SciencedirectDocument9 pagesResearch in Autism Spectrum Disorders: Sciencedirectcsepulveda10No ratings yet
- Sd. Down y Comunicación Referencial (Producción)Document10 pagesSd. Down y Comunicación Referencial (Producción)csepulveda10No ratings yet
- MSC Accounting & Finance in Southampton UniversityDocument11 pagesMSC Accounting & Finance in Southampton UniversityKemala Putri AyundaNo ratings yet
- Spencer - Van Etten Central School District: Reopening PlanDocument31 pagesSpencer - Van Etten Central School District: Reopening PlanWETMNo ratings yet
- Math g4 m4 Topic A OverviewDocument2 pagesMath g4 m4 Topic A OverviewzeynepNo ratings yet
- PESIT Calender of EventsDocument1 pagePESIT Calender of Eventsspandan.naik3428No ratings yet
- Final Project - BaluDocument94 pagesFinal Project - BalubalunriitNo ratings yet
- ENG-110 Composition I PDFDocument3 pagesENG-110 Composition I PDFaceventura72284No ratings yet
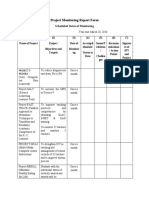
- Project Monitoring Report FormDocument3 pagesProject Monitoring Report FormAireen SiagaNo ratings yet
- DepEd music and arts lessonsDocument6 pagesDepEd music and arts lessonsCharmaine BayubayNo ratings yet
- Arturo Luz by Karl BelasaDocument4 pagesArturo Luz by Karl BelasaKarl BelasaNo ratings yet
- Case Pres Program 2Document2 pagesCase Pres Program 2Aira AlaroNo ratings yet
- Ged EssayDocument8 pagesGed EssayHein Htet ThuNo ratings yet
- During Reading Mini LessonDocument4 pagesDuring Reading Mini Lessonapi-489274706No ratings yet
- Cultural TranslationDocument16 pagesCultural Translationsaeedalimi0% (1)
- II. Report Description: On-The-Job Training (OJT) Is A Form of Training Taking Place in A NormalDocument5 pagesII. Report Description: On-The-Job Training (OJT) Is A Form of Training Taking Place in A NormalCharlene K. Delos SantosNo ratings yet
- Business Ethics - Module 2Document16 pagesBusiness Ethics - Module 2Aeio Kohen100% (1)
- Teacher's Interview QuestionsDocument13 pagesTeacher's Interview QuestionsGirlie Harical GangawanNo ratings yet
- Firm Growth TheoryDocument3 pagesFirm Growth TheoryChakraKhadka100% (2)
- Etika Kristen Penting dalam Pendidikan Karakter Era DigitalDocument18 pagesEtika Kristen Penting dalam Pendidikan Karakter Era Digitalanne yuliantiNo ratings yet
- A Sample A Recommendation Letter: February 2019Document3 pagesA Sample A Recommendation Letter: February 2019AbdullahiNo ratings yet
- The Role of Vocational and Technical Education - I. OlaitariDocument22 pagesThe Role of Vocational and Technical Education - I. OlaitarioedhieNo ratings yet
- Mismanaging During Storms - The Mike Harris and Tim Hudak Conservatives in OntarioDocument45 pagesMismanaging During Storms - The Mike Harris and Tim Hudak Conservatives in OntarioGregory BushNo ratings yet
- Professional Growth and DevelopmentDocument5 pagesProfessional Growth and Developmentapi-704201340No ratings yet
- Psi GoalsDocument3 pagesPsi Goalsapi-545998611No ratings yet
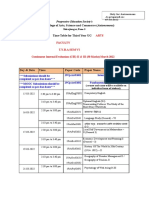
- Modern College Arts Time Table TYBA Sem VI March 2022Document2 pagesModern College Arts Time Table TYBA Sem VI March 2022Aniket SalveNo ratings yet
- FruitPersonality08 25 05 PDFDocument2 pagesFruitPersonality08 25 05 PDFSheni Ogunmola0% (1)
- ACIO Grade II exam questions and answersDocument34 pagesACIO Grade II exam questions and answersrahulNo ratings yet
- Trust in Schools Research From Bryk and SchneiderDocument4 pagesTrust in Schools Research From Bryk and SchneiderHari SreenivasanNo ratings yet
- Medicaps Application form-DrAmitAgrawalDocument6 pagesMedicaps Application form-DrAmitAgrawalDrAmit AgrawalNo ratings yet